|
By: Maria Trifas (CC '21)
Their Story:“We both got home from Columbia, and as we talked to friends over FaceTime and Houseparty, we realized how much free time everybody now had during quarantine. There was this underlying lack of purpose, and we were all itching to be useful. At the same time, we’re both in SEAS and had first-hand experience of the difficult transition to online classes. So, we could only imagine how hard this new learning format was for younger students. We realized that we could solve a small sect of this problem by becoming a solution to help younger students. It was important to us that there would be no financial barrier, and that we would take care of all of the logistics. So, if somebody wanted help or wanted to give help, whether a student or tutor, that they could immediately get involved.
It started out as an experiment, as we tried to see if we could really help some middle school children. We had 25-30 friends who worked with us to help put it together, doing outreach nationwide. We took a regional approach to spreading the word to students, reaching out to nearby schools from Brooklyn to the Bronx, as well as school systems in Texas and Virginia. We jumped from organization to organization and went on local news stations in LA and Boston to spread our outreach to students. Wherever we found parents who were struggling, we tried to reach out to them and offer flypaper as a service for their kids. We wanted to make sure that we were helping those who really needed it, and so we also went to hospitals in New York to offer our support to the kids of frontline workers. We had a sense of purpose and a reason to get up every day during quarantine to make a difference and help these families. Then, it just kept growing. We quickly realized how big of an impact flypaper could have for young students. We have college students from universities across the country who have volunteered to tutor, and middle-school tutees in a majority of the states. In total, we’ve completed over1500 hours of tutoring through the end of the school year, with hundreds of families on the site within 7-8 weeks of launching at the beginning of April. We found that kids needed support in different ways, even if it just meant the one-on-one engagement with another person. One mother told us that she had never seen her kid excited about learning, but after flypaper’s tutoring, he had a spark in his eyes to learn and engaged with a dusty science book that he’d never even picked up before. We built the original site on a more basic platform, but then it started quickly expanding. For us, when we see problems, we’re immediately driven to fix them. So, we didn’t see the high demand as a problem, but instead worked to provide for it. Now, we have a team of developers and are working with hackathons across the country to build upon our capacity. Early on, it was clear that we didn’t take the idea of kids’ education lightly; we wanted the students to get as much as they could from the academic help and mentorship. We wanted to build on kids’ interests and have them lead their own learning projects, with the help of tutors. After starting flypaper, we’re learning so much about different aspects of education that we didn’t think of before: what effective learning is, what engages kids, the difference between schooling and learning. Now, we’re doing a deep dive into understanding what those mean, and then making our future decisions based off of that. We want to continue to be helpful in a mindful way.” To learn more about flypaper tutors, visit their website, or follow them on Instagram, Facebook, and Twitter. They are temporarily pausing their tutoring services in order to plan ways to conscientiously grow and continue improving their platform to positively impact the learning of more students.
0 Comments
By: Arooba Ahmed (CC '23) Their Story:Vibhu:
"You get so used to checking in on patients room by room, being the person who knows their story really well and holding their hand when things are going wrong. Now, that ability to touch and connect is gone. So we made efforts to help via remote operations. I volunteered through CSSC—they have a student run hotline where people call in with symptoms and I provide resources and guidance. I would sit for a five hour shift and get many calls, some of which were heart wrenching. I had one really emotional conversation with a nurse who called in sobbing late at night. She said “I just took off my PPE and I got sneezed on by a COVID-19 patient, what do I do?” I was almost in tears with her while trying to talk through what happened and give her the number for occupational hazard. It was intense moments like these when I felt raw human emotion across a digital interface." Kendall: "I was also helping patients through the phone. I volunteer in the OB/GYN project, and there was a phone outreach program for postpartum patients. We would call them the day after they returned home to ask them how they were doing and check for red flags. It was similar to how it would be in the hospital. I had to have many difficult conversations over the phone; for example, depression and inter-partner violence screenings. It is uncomfortable as is, but over the phone when you can’t see each other, I had no idea what their reactions were. Sometimes there would also be a translator in between, which made it all even more disorienting. But in the end, it was so rewarding. Almost every woman who I called thanked me. Many of my patients were isolated in their homes alone, and sometimes I was their only form of contact." Vibhu: "As students, we also heard many stories from people still working in the hospital. There were doctors on twelve hour shifts without proper PPE watching patients die every single day. It was stories like these when I realized that I wanted there to be a space for frontline workers to share how they felt— hence why I started Faces of the Frontline. The world needed to bear witness to everything they were going through and I wanted to provide them with this platform for support. The first few weeks of the platform, there were days where I would mine through 200 stories, all from people who I would have never met, from fifteen different countries. It was beautiful to be able to connect with them through this platform. Hearing fellow doctors feel grateful about having a place to share their stories online and give them a moment of catharsis… that’s what gets me through." Kendall: "I edit the photo submissions for the stories on Faces of the Frontline. Some days, if a certain song came on while I was looking at a photo submission, I would burst into tears. The images really add to the reality of the stories. But the fact that I feel this way is important, because these people deserve for us to look back at their picture, and like Vibhu said, bear witness to what they feel. We also opened an artwork collection page on our website a month or two ago, and I collected a database of artists who support health professionals, like artists in the UK who are creating portraits to commemorate National Health Service heroes. We wanted to give these artists a sense of assurance that what they were creating made an impact on people. As someone familiar with both art and medicine, it's so interesting to see how they are interwoven and how art is being used now to express emotions that are unable to be expressed in any other way." Vibhu: "During these times of uncertainty, Faces of the Frontlines has not only helped to commend frontline workers, but it’s also given us a space to cope-- by connecting with the world and with its heroes on a far more expansive level than we could’ve ever expected." Visit https://www.facesofthefrontline.org/ to read stories from Frontline workers, submit a story, nominate heroes, view artwork, and more. Follow Faces of the Frontline on Instagram at @facesofthefrontline.
By: Hannah Lin (CC '23)

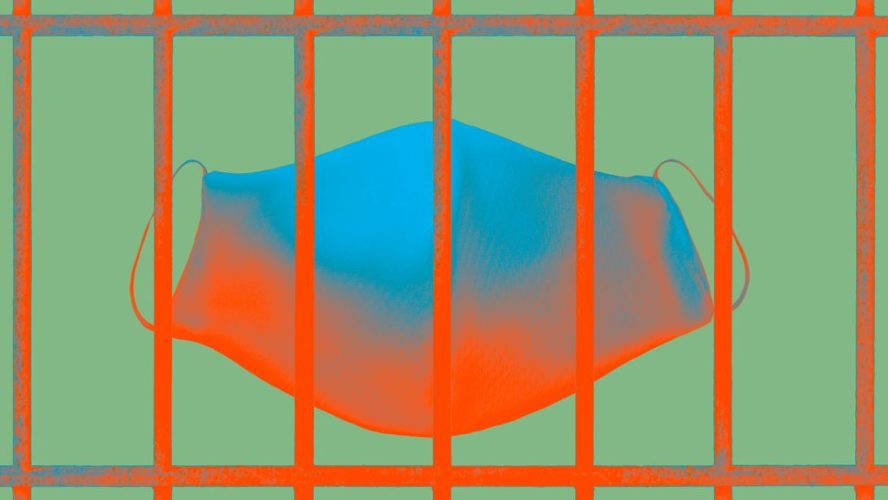
Cover illustration by: Vanessa Vasquez (SEAS '23)
Could you talk about your background? In my capacity as both a researcher on the faculty and also the director of the Center for Institutional and Social Change, I’ve been doing a fair amount of research and leadership development work related to reducing mass incarceration and, in particular, understanding and building the leadership of people who have direct experience with the criminal legal system. Recently, I’ve been working to gather and support the sharing of resources with lawyers, advocates, and others that are trying to support and advocate on behalf of people who are currently incarcerated and affected by COVID-19, as well as their family members. I’m also the vice president and policy director of an organization called the Broadway Advocacy Coalition. I’ve been doing a lot of work with that organization as well, related both to COVID-19 and also to the recent national reckoning related to race and racism. Before we jump into what you’re working on right now, could you give an overview of how the pandemic is shaping society from your legal perspective? I think the pandemic is amplifying and making visible forms of inequality that have been present really since the inception of our country but that have not necessarily been the focus of sustained public attention or concern, at least not in the last several decades. There are the obvious ways in which COVID-19 has affected people: social distancing and the things that we all know about, that everyone is experiencing in one way or another. What I’ve been observing is the profound and deep impact on communities that have already experienced disinvestment or marginalization and that are experiencing COVID-19 that much more intensively in every respect: more likely to have pre-existing conditions because of their connection to poverty or poor healthcare resources beforehand or conditions that are associated with inadequate support for housing and things like that.
just the failure of social policy that has relied on criminalization as a way to deal with issues or problems that would be much better dealt with through other strategies, such as public health strategies and strategies that engage people in the community.
That’s a lot of what COVID-19 has done. It has accentuated the impact that people have been experiencing in a way where the consequences are fatal. Because so much is shut down, because there are so many systems that are going to have to face new ways of doing work, and because of the visibility of what’s happening, I think COVID-19 has also opened up some real possibilities for dealing with these problems in a much more structural and systemic way than has been possible up until this point. What are some approaches that could be pursued?
people who are vulnerable, so the only solution that is really available is release. There’s beginning to be evidence that people who have been incarcerated and have been released really did not require incarceration in the first place.
The mechanism to release people who are incarcerated who are threatened with serious illness or death exists, even in the current system, but many public officials have been unwilling to use them, whether it’s judges, the governor, or the commissioner. The consequences, I think, are part of what really needs to be documented: the consequences of essentially tolerating conditions that public health officials have made clear will increase death rates within prisons and jails. I think the level of public attention around the structural problems that are built into our current approach to incarceration opens up the possibility of really shrinking the footprint of prisons and jails and moving more toward restorative justice type approaches that are grounded more in the community. There is evidence of the lack of capacity of the prison and jail complex to navigate something like a pandemic and the disproportionate impact not only on people incarcerated but also on everyone who has contact with those people—people who are working in prisons and jails, their family members, et cetera. As the consequences for those communities become more visible and there’s more public attention focused on those, there opens up the possibility for having really serious conversations going forward.
that are in the wings as we grapple with the complete failure of the systems as they are currently operating to manage in this crisis and the mobilization of communities that I think are going to stay engaged and create the public pressure that’s needed to shift the emphasis from incarceration to public health.
Can you talk about the research you are working on right now? A bunch of the research that I’ve been supporting has been in collaboration with a group of advocates, a national organization that’s called Zealous, which brings together public defender offices from around the country. Together with Columbia law students, the Bronx Defenders, and UCLA’s COVID-19 project, we have been gathering and systematically analyzing cases across the country that deal with COVID-19 and creating an online site that is searchable and will be available to advocates and researchers. It allows patterns in decision making on the part of judges, corrections officials, and public officials to be identified, compared, and analyzed in relation to factors such as geography, the nature of the crime that someone is incarcerated for, what their pre-existing health conditions are, how long their sentence has been, and other variables. Then, we can look at what has happened and understand what it is, in exactly the same situation, that predisposes one judge to essentially step back from exercising discretion in a way that would preserve human life as compared to another judge who really steps up to the situation. Additionally, we’re trying to use the best available resources to advocate on behalf of people who are seeking either release or better health and screening mechanisms while they’re in prison. People, once they’re released, are coming home to really difficult circumstances, so we’re also trying to understand what the needs of people are once they leave prison and what is available, both legally and socially, to support those individuals.
This is all in process right now. There is a public Google form, an Excel spreadsheet that has all of the case data that has been analyzed thus far. That will be publicly available. For the website, a portion will be publicly available and a portion will be password protected. Something that has been very gratifying for me is that there are about 25 Columbia law students that have been working on this project, either volunteering, getting their pro bono credit, or doing this as a summer job. Columbia law students have been doing a lion’s share of the case analysis that has been populating this site to be available for the public. It’s important to mention what’s happening in the world right now alongside the pandemic, which is the fight against anti-Black racism and for justice, for equality. I wanted to hear your thoughts and observations on the last month, especially from your perspective as someone who has made a career out of focusing on racial and gender biases and tackling institutional change and structural inequalities in employment, in higher education as well. For me personally, the last month has been wrenching and sobering, just to be re-witnessing the pattern that’s repeated over and over again and in a way that is so painful and damaging particularly to Black people, who have been living with this same pattern. It’s also been a time of introspection. I do work in this area and this is something I spend a lot of time on. I’ve been spending the last three years working with the Massachusetts Trial Courts to help them build their capacity to address race and bias in the Trial Court, and I've been spending the last four months pulling together a guidebook and materials. Even with all of that, I’m wondering and asking the question, “Are there ways in which I can use the position that I am in either to address these issues or support the work of organizations led by people of color to advance anti-racism? What are the ways in which I really need to step up and how do I do that in a way that doesn’t occupy the room that really needs to be respected for people who have directly experienced this kind of racism?” It’s been an introspective and sobering time.
I’m seeing colleagues both in my own law school and in other law schools that are using the language of racism, anti-racism, systemic racism, and accountability in ways that I’ve not heard before. I’m seeing students who are really equipped to press for change in a very sophisticated and impressive way. So I feel simultaneously angry and despondent and also hopeful for conversations about really fundamental change both in the criminal justice system and in higher education and in politics. I am writing a book that grapples with the paradoxes built into efforts to move white institutions toward anti-racism. I think the big question is going to be how we will sustain this kind of inquiry and how we will avoid cosmetic short term solutions that will just make people feel good or feel like they’re taking action. How we will enable people to understand why this is a concern that is critical for everybody. It’s critical for the health of our democracy, it’s critical for the flourishing of people in predominantly white institutions and the support of people who have been working in predominantly Black or other racial institutions.
What gives you hope for the future? I think the biggest thing that gives me hope is that I see really strong, committed, effective leadership coming from your generation, from my law students, from formerly incarcerated individuals who have organized in ways that really highlight both their capabilities to lead change, their knowledge, and the kind of ground truth that they bring. I think that’s the thing that gives me the most hope: seeing the kind of mobilization and leadership among the people who really need to be at the forefront of holding our institutions accountable and pushing this change forward. That makes me hopeful. I also see an openness to accepting responsibility on the part of at least some in positions of power and influence who have never done that before. I also see the combination, which can hopefully be sustained, of really strong leadership that really pushes for and holds people who are in positions of power accountable and openness to sharing power, stepping back, making change, and then putting things on the table that just need to be addressed squarely that involve race, racism, and dysfunctional institutions that need to be rebuilt from scratch, such as the prison system, the system of mass incarceration. I see ideas that were treated as beyond the pale even a few years ago that are on the table now. To the extent that we are willing to face into our failures and do something to change in a sustained way, there will be hard work. There will be a lot of pushback, there will be a lot of backsliding, but I think there’s hope for much more transformational change to grow out of this period of suffering. Interview Highlights: The Effects of Asthma on COVID-19 Outcomes With Stephanie Lovinsky-Desir6/22/2020
By: Hannah Lin (CC '23)

Cover illustration by: Zoe Chan (CC '22)
The following is a heavily condensed version of the full interview. If you're interested, read more here. Could you talk about your background as a researcher and your research prior to COVID-19? I do a lot of research on asthma, mostly asthma in children, and I’m also very interested in health disparities. I’ve been very much inspired to investigate sources of disparities in asthma outcomes, particularly in minority and underrepresented populations in urban communities. Given your expertise and prior work, it must have been a pretty natural step, once the pandemic came around, to switch the course of your research to analyzing COVID-19 in people with asthma. Absolutely. Not only do I do research in this field, I take care of children with asthma. As the pandemic started to hit, there was this question of, “are my pediatric patients or any patients who have asthma at greater risk for having bad outcomes from COVID-19?” It was a natural question that we felt we were in a great position to be able to answer, being at the epicenter of the COVID-19 pandemic. Could you talk more about your COVID-19 research and the work you’ve been doing in the past couple months?
We were really interested in seeing if having an underlying diagnosis of asthma set people up for worse outcomes. Basically, the punchline is that we didn’t see any significant differences in those individuals who had an underlying diagnosis of asthma compared to those individuals who didn’t have a diagnosis of asthma. It’s really important, though, that I recognize one of the limitations: we’re not able to say from this analysis if having a diagnosis of asthma puts you at greater risk for actually getting COVID-19.
While we didn’t see any differences even when we accounted for the different comorbidities and obesity, we did see that the incidence of asthma among those hospitalized with COVID-19 was a bit higher in that younger age group (those less than 21 years old)—about 24% of them had a history of asthma, whereas in the older patients that were older than 21 and up to 65 years of age, the prevalence of asthma was about 13%. What do the next steps look like for your research? I have a couple of other things in the pipeline related to COVID-19, although I never imagined myself to be a COVID-19 researcher. I don’t think I ever imagined myself to be a researcher during the time of a global pandemic. I think, in science, we have to go where the questions take us, so right now, the question is: how is COVID-19 affecting our population and the people we care for?
I was also a part of another effort looking at health disparities in COVID-19. We have a manuscript that’s currently awaiting publication as well. It’s less data-specific and more theoretical frameworks of how racism sets certain populations up for worse outcomes of disease and giving information to our colleagues on why that might be. It has some action items that people can work towards to help mitigate health disparities as they relate to COVID-19.
For the general public, as a medical doctor, what are the big pieces of advice you want to shout from the rooftops? Let me tell you: with everything opening up right now, people who have been hibernating for many months, and people who are just itching to get out there and be connected with their loved ones, doing things that make them feel normal again because there is nothing that has felt normal in the last three months, I’m a little nervous. What I want people to keep in mind is that this was bad. This was really, really bad. It didn’t affect everyone equally, and I think the fact that some people felt it harder than others adds to why certain populations might feel more and more comfortable as we open up.
Lastly, to end with some optimism, I always like to ask: what gives you hope for the future? Related to your research, science more broadly, or life in general. I think one of the things this pandemic has taught us is resilience. I think so many of us were forced, pushed, and shoved into a setting that none of us thought we would be comfortable with, but somehow we’ve managed to survive and thrive. I think that is what gives me the most hope: knowing that we are a resilient group of people and when thrown in an environment
By: Hannah Lin (CC '23)
Could you talk about your background as a researcher and your research prior to COVID-19? I do a lot of research on asthma, mostly asthma in children, and I’m also very interested in health disparities. I’ve been very much inspired to investigate sources of disparities in asthma outcomes, particularly in minority and underrepresented populations in urban communities. One of the areas I’ve worked on a lot in recent years is looking at air pollution exposure and, more specifically, the effects of being physically active in polluted communities. We know that physical activity is really good for the lung health of all individuals, but sometimes if you're active in areas where there’s high pollution, there’s a potential that you might be inhaling more pollution particles, and that might mitigate the effects of physical activity. This is the area where I’ve spent most of my time studying in the last several years. Given your expertise and prior work, it must have been a pretty natural step, once the pandemic came around, to switch the course of your research to analyzing COVID-19 in people with asthma. Absolutely. Not only do I do research in this field, I take care of children with asthma. As the pandemic started to hit, there was this question of, “are my pediatric patients or any patients who have asthma at greater risk for having bad outcomes from COVID-19?” It was a natural question that we felt we were in a great position to be able to answer, being at the epicenter of the COVID-19 pandemic. Could you talk more about your COVID-19 research and the work you’ve been doing in the past couple months? We have one project that we put together and we’re waiting to hear back from a journal on whether it was accepted for publication. It’s looking at all of the patients that came into the Columbia University Medical Center, so that’s over at our adult Milstein Hospital, at the Morgan Stanley Children’s Hospital, and at the community hospital up at the Allen Pavilion. We looked at all people who came in who had COVID-19 and were younger than 65 years of age, and we compared those who had diagnoses of asthma before they came in for their hospitalization and those who did not have asthma. We were really interested in seeing if having an underlying diagnosis of asthma set people up for worse outcomes. We looked at mortality, intubations, and how long people were hospitalized. Basically, the punchline is that we didn’t see any significant differences in those individuals who had an underlying diagnosis of asthma compared to those individuals who didn’t have a diagnosis of asthma. It’s really important, though, that I recognize one of the limitations: we’re not able to say from this analysis if having a diagnosis of asthma puts you at greater risk for actually getting COVID-19 because, as you know, we don’t have universal testing here and we didn’t have it specifically at the beginning of this pandemic. A select group of people who were sick enough to be hospitalized were the ones early on who were actually able to get a COVID-19 test. We can only really say that if you were sick enough to either be hospitalized or die in the emergency room in one of those three hospitals I mentioned, then your overall outcome, having had a diagnosis of asthma, was not significantly different than those people who did not have asthma. We also looked at people with asthma and underlying comorbidities including heart disease, high blood pressure, and diabetes, because those have all been associated with worse outcomes of COVID-19. We also looked at people who had obesity, comparing asthmatics with obesity versus non-asthmatics with obesity. Then, we looked at children, since I’m a pediatrician, so I’m really interested in that younger-than-21 age group. While we didn’t see any differences even when we accounted for the different comorbidities and obesity, we did see that the incidence of asthma among those hospitalized with COVID-19 was a bit higher in that younger age group (those less than 21 years old)—about 24% of them had a history of asthma, whereas in the older patients that were older than 21 and up to 65 years of age, the prevalence of asthma was about 13%. Have you faced any setbacks in your COVID-19 research? Yes. I will say that it was really a tedious task to gather these data. The first issue was how we were going to find the data, how we were going to get access. We knew that there were hundreds and hundreds of patients coming in, but trying to figure out the best way to access those medical records was a bit of a challenge. We started by using the clinical data warehouse, for which Columbia University has a team of people who are able to pull data from electronic health records for reasons like this, to be able to do scoping analyses in large groups of patients. But the one thing we realized early on was that the definition of asthma was not very good when we used that data source, so while we were able to get the numbers, we had about 1400 patients who we realized fit our criteria of being hospitalized in our centers and being younger than 65 years of age. I assembled a team of amazing trainees that helped me and we went through the arduous task of going through each of these 1400 medical records to confirm the diagnosis of asthma and to look for comorbidities. That was a bit painstaking. There was a lot of time spent in terms of going through each chart and looking through the notes, orders, medication lists, and things like that. But I do think that was the only way for us to get really good data that we could believe in and feel confident about the message that we’re actually sending out of this study. What do the next steps look like for your research? I have a couple of other things in the pipeline related to COVID-19, although I never imagined myself to be a COVID-19 researcher. I don’t think I ever imagined myself to be a researcher during the time of a global pandemic. I think, in science, we have to go where the questions take us, so right now, the question is: how is COVID-19 affecting our population and the people we care for? I’m working with colleagues in the allergy/immunology division to do a similar study looking at allergic disease and immunodeficiencies and differences in outcomes in hospitalized patients with COVID-19. I’m also working with another group of really brilliant researchers, some within Columbia and some outside, to look more at the health disparity issues associated with COVID-19, and we’re really interested in healthcare access and delivery. We’re hoping to combine data across a few centers to see if we can get at whether certain populations in New York City are more disadvantaged in terms of their access to care and the quality of care that they receive during this global pandemic. Those are the projects related to COVID-19 that I have on my plate right now. I was also a part of another effort looking at health disparities in COVID-19. We have a manuscript that’s currently awaiting publication as well. It’s less data-specific and more theoretical frameworks of how racism sets certain populations up for worse outcomes of disease and giving information to our colleagues on why that might be. It has some action items that people can work towards to help mitigate health disparities as they relate to COVID-19. That’s what I’ve been doing the last couple of months and where I see the next couple of months going, but I do have a lot of work ongoing from before COVID-19 that I’d like to continue focusing my efforts on. You sound so busy just from that, but you don’t only do research. You’re a physician scientist, so you are obviously a physician as well. Are you seeing patients in person or over telemedicine right now? At the beginning of the COVID-19 pandemic, we mostly transferred all of our outpatient care to telemedicine, which was an interesting experience, and I think we’ve been able to provide good quality care to our patients who really needed us in the middle of a pandemic when people were really scared to come into the medical center. I’m continuing to see patients via telehealth both here at Columbia and at a practice that I share with a colleague at Harlem Hospital, where we do community-based pulmonary care. But our doors are now open to see patients here at Columbia as well. We’ve made a lot of efforts towards keeping our hospital COVID safe to protect our patients and our teams. I’ve also been attending on inpatient service, rounding on our inpatients and doing consults during this whole pandemic. For the general public, as a medical doctor, what are the big pieces of advice you want to shout from the rooftops? Let me tell you: with everything opening up right now, people who have been hibernating for many months, and people who are just itching to get out there and be connected with their loved ones, doing things that make them feel normal again because there is nothing that has felt normal in the last three months, I’m a little nervous. What I want people to keep in mind is that this was bad. This was really, really bad. It didn’t affect everyone equally, and I think the fact that some people felt it harder than others adds to why certain populations might feel more and more comfortable as we open up. So I think what I want to shout from the rooftops is: please, people, be thoughtful, be safe, and be careful. Now that we know what COVID-19 is and we know what strategies have helped to taper its severity in terms of its effects on our communities, we cannot abandon the things we’ve been doing to maintain social distancing, not gathering in large crowds, wearing our masks when we are around other people, and not being around other people when we’re feeling sick and ill. These are really, really important measures because we’re all a bit scared of what is going to happen in the fall. We don’t know, so we need to do our best right now to protect ourselves and to protect everyone around us. Lastly, to end with some optimism, I always like to ask: what gives you hope for the future? Related to your research, science more broadly, or life in general. I think one of the things this pandemic has taught us is resilience. I think so many of us were forced, pushed, and shoved into a setting that none of us thought we would be comfortable with, but somehow we’ve managed to survive and thrive. I think that is what gives me the most hope: knowing that we are a resilient group of people and when thrown in an environment that is unfamiliar or unconventional, we have figured out ways to adapt and continue to thrive. I think that’s an important thing to recognize in all of us—that we’re still here, we’re still doing okay, we’re still committed to our mission of providing great care, we’re still committed to our patients in terms of understanding what it is that’s affecting them and how we can improve health overall. I find that to be incredibly inspiring, how we’ve all managed through this and here we are on the other side, still standing, many of us. That’s hopeful for me. Full Interview: Processing 35,000 COVID-19 Patient Samples In 3 Months With Álvaro Cuesta-Domínguez6/18/2020
By: Hannah Lin (CC '23)
Can you introduce yourself? My name is Álvaro Cuesta-Domínguez, and I am an associate research scientist in the physiology and cellular biophysics department. My research focuses on the interaction between the bone marrow microenvironment (specifically osteoblasts, cells of the bone) and hematopoietic stem cells in the context of leukemia. In my lab, we have a collaboration with a clinical researcher at Columbia and we biobank bone marrow cells from patients with leukemia. You’re the founder of CRAC (Columbia Researchers Against COVID-19). Could you talk about how you came up with the idea? This is going to get personal. As a member of the LGBTQI+ community who was born in 1981, I have lived all my life with the HIV/AIDS pandemic in mind. When I heard that there was another pandemic hitting a vulnerable population, I felt like I needed to step up and do something. So when we got the notification from the university saying that we had to ramp down research (we were not able to perform any research if it was not related to COVID-19) I thought that most researchers like me would have “free time” (in our weekly schedule, 50% of our time goes to new experiments and 50% of the time is analyzing results, attending seminars/meetings/conferences, and other non-experimental work) to help with coronavirus testing, as this relies on PCR, a routine molecular biology technique. This was my idea when we started CRAC: organizing a group of researchers that would be willing to help in testing for the virus. I sent an email to Dean Goldman and other officials of the medical center, and got a very good response. There were a lot of regulations regarding testing, since you need to be clinically validated for all these things. There were also a lot of regulations about researchers on visas performing clinical or diagnostic work. About one week after we launched the group and started recruiting volunteers, we started getting calls from different departments and levels of administration at Columbia asking for help in different capacities. I learned that the pathology department was starting a biobank of COVID-19 patients on campus and because of my lab experience, I thought that I could help and so I was deemed the leader of the biobank project. Could you explain what biobanking means? Biobanking is processing and cryopreserving (storing collected samples in freezers at -80 degrees) so that researchers can access these samples and perform research to gain insight into unknown aspects of the virus and the diseases that it causes. For example, let’s say we have one tube with 10 milliliters of blood of a COVID-positive patient. What we did was pipette different components of this blood (serum, plasma, mononuclear cells) into different tubes (in lab jargon, “aliquot”) and then store them at -80 degrees. You started on March 31st, when New York was in the peak of the pandemic. What did you have to do to get this off the ground, and did you face any setbacks during that time? The first thing was finding a space. This was achieved by Dr. Hod’s lab. He was actually going to move his lab to another location, and when this happened, he decided to use his new space as the new COVID-19 lab. In this space, not only have we been collecting the samples and preserving them, but also the serological assays validation, one of Dr. Hod’s projects that CRAC also helped on. After the space was chosen, the next thing we needed to consolidate was the workflow. For this, I was working with Dr. Francesca La Carpia and Sebastian Fernando, the two main people in Dr. Hod’s lab who have been supervising the volunteers. I shadowed them for a day and a half to see what was needed, and this helped me understand what the requirements were for the people I had to lead. A lot of challenges arose after I started recruiting people, the first one being biosafety. Not only were we asking people to leave their homes and families, we were also asking them to be in front of samples that had the potential to transmit the virus. What we did and what we thought was the best idea was to divide the weekly schedule in four hour shifts so that every volunteer would only do four hours a week: a single exposure on just one day for just four hours. We were able to do this because CRAC had, at that point, almost 500 volunteers, so it was easy to find a big group of people with the proper training and expertise. Our project started with 8 volunteers, and eventually we expanded to 18 working in the morning and afternoon. Not only was the aim to reduce possible transmission, but also to reduce burnout from a task that is very, very tedious. We used racks of 81 tubes that had to be “aliquoted” into 2 or 3 cryoboxes, so it’s basically a robot task. Those were the initial challenges that I faced as the manager of the group. We’ve been providing all the necessary PPE, and we take great pride in the fact that, as of today, no one has developed symptoms or gotten sick. In the beginning, I was really scared. I’ve had a lot of sleep problems thinking that someone could get sick because of their work in the biobank, and I am really glad that no one did. The project ended June 5th, and your team collected 35,000 samples, which is just amazing. Was it always going to be a 2 month project? From the CRAC perspective, we were an emergency response team. We had to assemble this infrastructure in a record amount of time because we either did this or we lost these samples. And these samples are gold. My PI has always been very vocal about the value and worth of patient samples, so I knew we really had to push to get this going and get it off the ground. Apart from the 35,000 samples, which is amazing, we donated 423.5 hours of work. This speaks a lot about the people that I’ve been working with: they’re not only great scientists, but getting to know them personally has been really touching. The fact that they were willing to get out of their apartments and do this really speaks a lot about them and it makes me proud to be part of this research community. What are you focusing on now, and what lies ahead in the future for you? Apart from the biobank project, CRAC has been running another 22 projects. Other volunteers have been helping with the serological assays validation; another group was assisting New York Presbyterian Hospital with scrubs distribution, and helping build the two field hospitals that were running during the peak. There’s another group organizing the weekly COVID-19 symposium for Columbia researchers and guest researchers. That group is still working, but most of the projects are already completed. There’s still an ongoing discussion on what CRAC is going to be doing. As for me, I’m ramping up my own research because I’m in my fourth year of postdoc here at Columbia and I’m about to submit my story. I need to finish a couple experiments. I’m really looking forward to going back to this “new normal.” You were a co-author of an op-ed earlier this year calling for Columbia to increase pay for postdoctoral and associate research scientists. Can you talk a bit about that? Yes, I’ve been helping to organize the postdoc and associate research scientist union at Columbia. I think we can all agree that postdocs are the backbone of research at Columbia. We bring a lot of value, prestige, and money through funding in grants. I think it’s as much as 1 billion dollars every year. If you look at the salary ranges of our peers in the New York City area, we are, without any doubt, the researchers with lower salaries. We’re only asking to have fair salaries and fair compensation that allow us to live in one of the cities with higher cost of living. It’s as simple as that. We’re asking for comparable compensation to other institutions in New York. This really impacts the quality of our research because many of us, at some point, have had to worry about paying rent, childcare or medical bills, and this really takes our focus out of our research. So fair compensation and increased benefits for postdocs at Columbia would have a very positive impact for postdocs so that we can focus on what really matters: our experiments and projects. How is COVID-19 now affecting your efforts to fight for fair compensation? The union and the university signed a no strike-agreement when we got recognition for the union. We have spent 16 months in negotiations over our conditions, and the deadline was April 9, I believe. The peak of the pandemic was exactly at that time, so bargaining was extended and we still are in this process. It has impacted us in the sense that we should already have a contract by now. The university has made some advancements in the negotiations, but we feel like they haven’t really moved in two core aspects of our demands. One of the them is compensation, and the other is a timely grievance procedure for bullying, harassment, and all sorts of discrimination. Note: Since the date of this interview, the union has reached a tentative agreement. Read more here: https://columbiapostdocunion.org/contract-negotiations/cpw-uaw-status-negotiations-2020/. To end with some optimism: what gives you hope for the future? I am very optimistic. Maybe I’m too optimistic to be a scientist! [laughs] I’ve seen really good things during the response to the pandemic. I think that science is definitely changing. We have seen way more collaboration and cooperation instead of competition. We have seen many research groups joining forces, collaborating, sharing reagents, plasmids, and all sorts of resources. My hope is that this will not just be for the pandemic and that we will be able to learn from this experience to really push science forward in a more collaborative way. As for the outpouring of solidarity from all the researchers that we recruited, we had more than 700 people that were willing to do anything, from labeling tubes to folding scrubs—we’re talking about people who have been doing science for more than 10 years and have a lot of experience. I think that really speaks a lot about our researcher community and the commitment that we have to science and society at large. 
Cover illustration by: Arooba Ahmed (CC '23)
Interview by: Hannah Lin (CC '23)
The following is a heavily condensed version of the full interview. If you're interested, read more here. You’re the founder of CRAC (Columbia Researchers Against COVID-19). Could you talk about how you came up with the idea?
getting calls from different departments and levels of administration at Columbia asking for help in different capacities. I learned that the pathology department was starting a biobank of COVID-19 patients on campus and because of my lab experience, I thought that I could help and so I was deemed the leader of the biobank project.
You started on March 31st, when New York was in the peak of the pandemic. What did you have to do to get this off the ground? The first thing was finding a space. After the space was chosen, the next thing we needed to consolidate was the workflow. A lot of challenges arose after I started recruiting people, the first one being biosafety. Not only were we asking people to leave their homes and families, we were also asking them to be in front of samples that had the potential to transmit the virus. What we did was divide the weekly schedule in four hour shifts so that every volunteer would only do four hours a
The project ended June 5th, and your team collected 35,000 samples, which is just amazing. Was it always going to be a 2 month project? From the CRAC perspective, we were an emergency response team. We had to assemble this infrastructure in a record amount of time because we either did this or we lost these samples. And these samples are gold. Apart from the 35,000 samples, which is amazing, we donated 423.5 hours of work. This speaks a lot about the people that I’ve been working with: they’re not only great scientists, but getting to know them personally has been really touching. You were a co-author of an op-ed earlier this year calling for Columbia to increase pay for postdoctoral and associate research scientists. Can you talk a bit about that? Yes, I’ve been helping to organize the postdoc and associate research scientist union at Columbia. I think we can all agree that postdocs are the backbone of research at Columbia. We bring a lot of value, prestige, and money through funding in grants. If you look at the salary ranges of our peers in the New York City area, we are, without any doubt, the researchers with lower salaries. We’re only asking to have fair salaries and fair compensation that allow us to live in one of the cities with higher cost of living. It’s as simple as that. This really impacts the quality of our research because many of us, at some point, have had to worry about paying rent, childcare or medical bills, and this really takes our focus out of our research. So fair compensation and increased benefits for postdocs at Columbia would have a very positive impact for postdocs so that we can focus on what really matters: our experiments and projects. Note: Since the date of this interview, the union has reached a tentative agreement. Read more here: https://columbiapostdocunion.org/contract-negotiations/cpw-uaw-status-negotiations-2020/. To end with some optimism: what gives you hope for the future?
for more than 10 years and have a lot of experience. I think that really speaks a lot about our researcher community and the commitment that we have to science and society at large.
By: Julienne Jeong (CC '21)
Their story:“One of the most important realizations that I had early on was that in the face of a crisis, there was a place for everybody to help. It wasn’t a matter of finding a position that I was uniquely qualified for, but it was a matter of just getting involved. In academia, we are always told to take time to prepare and be certain of our decisions, but this crisis has shown me that I, along with the rest of the world, will never be prepared for most things. I’m not a science major, I’m not on the pre-medical track, and I don't even know where the heart is located in the body. Yet, I figured things out because I realized that things needed to happen and we couldn’t wait around for people to do them. I think that actually worked to my advantage because while a lot of people were reaching out to similar medical organizations for PPE donations, I thought of places that used PPE in other industries. As an English major, I knew that rare books and manuscripts had to be carefully handled because many of the texts are hundreds of years old, so I reached out to the Columbia Rare Books and Manuscripts Library and they actually donated over 30 boxes of gloves, masks, shoe covers, and full body covers. It was only our second donation, but it is still the largest donation we have ever received. I ran down the street in the pouring rain and I showed up to the back of Butler Library with a small wagon to carry the PPE donations from 116th to 89th street. The librarian was waiting with eight moving boxes full of nitrile gloves, and he told me, “This probably won’t fit.” He was right. That was one of the first moments that I thought, “Ok, we’re doing something.” Our first priority was to donate to hospitals and clinics that were being underserved by the existing PPE network. We’ve also donated to women’s shelters, soup kitchens, and trans healthcare facilities, a few of which were close to shutting down as a direct result of PPE shortages. These shortages weren’t just affecting cases of COVID-19 but they were impacting people who needed PPE for other important uses, like getting access to hormone therapy or receiving basic healthcare needs. Now, we have warehouse coordinators and drivers, most of whom we found on Facebook Queer Exchange and are uninvolved in medicine. They’re just regular people with cars, bikes, and motorcycles who offer to transport materials to nearby facilities. Sometimes, I’ll run with a backpack full of masks myself. There were definitely moments when I wanted to sit and watch Desperate Housewives for four hours with my eyes glazed over, but I knew that this was work that needed to get done. Every pair of gloves we donated mattered, and that was what pushed me through.” To support MedSupplyDrive, please share this story and learn how to get involved or donate on their website. Follow MedSupplyDriveNYC on Facebook and on Instagram @medsupplydriveNYC 
Cover illustration and gif by: Zoe Chan (CC '22)
Interview by: Makena Binker Cosen (CC '21)
The following is a heavily condensed version of the full interview. If you're interested, read more here. Could you describe your COVID-19 research at the moment? Our team has been running models that project COVID-19 outcomes for New York City, U.S. counties, and the entire country, as well as for China. For example, back in January, we started by estimating how many people had undocumented infections and how contagious they were. Our goal is to understand the pandemic’s epidemiological characteristics: its distribution, patterns, and determinants of health across populations. This type of information can help us identify what public health interventions different places ought to adopt.
people get more relaxed, businesses open, and there is less compliance with social distancing and face-mask wearing. Another scenario might be that the transmissibility will stay constant, if everyone stays on their toes. Modeling these scenarios allows us to identify the scope of possible outcomes and to understand how sensitive the virus is to specific interventions. In turn, this helps us determine which measures we ought to enforce in different places.
What biases do you face in data collection? First off, not everybody is tested. Many COVID cases go undocumented, and deaths are undercounted. In fact, someone from a hospice in rural Georgia reached out to me, saying that they used to get one or two sepsis cases each year. Now everybody there is dying of “sepsis” and none of them have been tested for COVID. It’s likely that they’re all COVID patients, just not known to be.
On top of this, there are changes in reporting and testing practices over time. We don’t have access to information on the microscale processes that might be supporting or not supporting transmission locally.
How do your models address these biases? Our job is to use models that explicitly allow and account for biases in the data. Observations are not the Gospel. There is some unknown truth out there that we’re trying to estimate better by using both these models and the observations in conjunction with one another. Because there’s a lengthy lag between someone acquiring the infection and them being counted as a confirmed case, our main blind spot is that we don’t know what happened over the last ten days. We update our projections twice a week using new information from the last three or four days, and we also change our scenarios as we consider new behavioral changes. It’s really important in this situation to be very responsive. When there are outbreaks taking place, we would like to see states and communities responding aggressively. Unfortunately, that has not been the case. What are some key interventions that you’ve seen lead to an effective response to COVID?
One of the best examples to look at is South Korea, since it is a densely populated, modern country well-connected with the world economy, and people fly through it all the time.
Since then, they’ve further reopened businesses, houses of worship, and nightclubs, among other non-essential services. The opening of nightclubs was associated with a cluster of outbreaks, around forty cases a day. Now, if they had forty cases per day for a thousand days, that would be forty thousand cases. If we assume there are about ten times as many infections overall as there are cases, which is probably a high number for South Korea considering how well they test, that would be 400,000 people infected in the next three years, roughly. That is less than one percent of their total population. In their new normal, with a reasonable economy, maintaining their unemployment rate at four percent, South Korea could hold on for three years while the world tries to develop an effective vaccine or therapeutic treatment for COVID-19. What’s more, they could deploy it before 99% of their population is ever infected with the virus. Now, South Korea has a little bit more than one-seventh of the population the United States has. Forty cases per day there would approach 280 cases per day here. Right now, the United States has about 20,000 cases per day. We’re nowhere near their numbers and we’ve disrupted our economy and skyrocketed unemployment. We’re not alone. A lot of countries have done the same. Right now, we seem to be ignoring the fact that this can take off exponentially again. We may be catching a break in summer because the virus may be somewhat less transmissible then. However, if we’re really complacent about this and we’re not willing to reimpose shelter-in-place methods, this virus will run over us. Has your team modeled how protests and the response to protests may influence COVID-19 outcomes?
On the other hand, bringing people together may provide more opportunities for transmission and there have been locations where people are not wearing face masks at all. That’s more concerning. This is not to diminish the need for the protests. That is a choice and these issues are very important, equally important, if not more important, and they are connected to public health issues as well.
Cover illustration by: Arooba Ahmed (CC '23)
Interview by: Hannah Lin (CC '23)
The following is a heavily condensed version of the full interview. If you're interested, read more here. Let’s back up to the pre-COVID days. You two are the principal investigators, or PIs, of a study called the CONCERN study. Can you talk about that? Rossetti: It stands for “Communicating Narrative Concerns from RNs.” Essentially, we know that nurses are at the bedside in the hospital with patients observing them the most of any clinicians in the hospital. They observe when patients are not doing well, they observe when patients have signs and symptoms before vital signs change that indicate that they are going to have a potentially bad event in the hospital, such as a cardiac arrest or death. 
We are actually able to detect when nurses have this level of concern about a patient because we look at how they record information about the patient. They record information more frequently, because they’re going into the patient’s room more frequently, and they’re paying close attention to certain things. So we can see that pattern in the electronic health record (EHR) and we’re able to use different data science techniques to identify early when a patient’s at risk for deterioration for a bad event. We can use that information in a prediction model so that the entire care team can be better aware earlier that the patient is at risk. Your COVID-19 project is called “Scaling up for Surge Capacity and COVID-19 Patient tracking in the Electronic Health Records: Leveraging Healthcare process modeling”. Can you break that down? Cato: The idea behind this project is that during a community-wide emergency like COVID-19 or 9/11, where you have lots of people using hospital resources at the same time, there are a couple things that happen. What we were trying to do was help the hospital track patients in a more automated way to understand how many really sick patients were on ventilators.
tagging it as that, because then you’ve led yourself to a human error. What we wanted to achieve was two goals: one was to reduce that human error, but two, we wanted to automate it so we could have it in real time.
How were your results? Cato: We had really good results; our precision was about 99%, which means that if you had 100 really sick patients, our method would know that almost 100 of those patients were really sick patients. The take home message from that is that human beings aren't right all the time. What are your next steps in terms of COVID-19 research? Cato: One is the resource mapping that I was just talking about, the bed tracking. The idea is that we want to be able to build applications that people can use throughout the country and world where this can happen automatically and a human being doesn’t have to go and count the resources every day.
Rossetti: Another related issue that we were looking at is which of our patients are on ventilators. Ventilators were a huge issue during COVID. The information about ventilators is recorded in some ways that makes it complicated to identify the precise time at which a patient started on a ventilator and stopped on a ventilator. We’re able to apply this healthcare process modeling technique in order to have more accurate timeframes for when patients are on ventilators.
To end with some optimism, what gives you hope for the future? This can be related to your research, science more broadly, or life in general. Rossetti: So many things have occurred in the last few months and weeks. I think we’re seeing a lot of change—needed change and good change that needs to happen in the world regarding Issues around racial disparities and systemic bias. These conversations need to happen and are happening, so I see that movement being escalated, and hopefully, will continue. Related to the specific work that I do, if you look at what happened during the COVID response, we have amazing clinicians that were and are our heroes. We actually can show from the health care records the decisions clinicians are making for their patients, and the expertise that they’re applying is really amazing. We want to continue our work and continue perfecting these data science techniques, these healthcare process models, to really show the great work that clinicians are doing.
I also feel very optimistic about how, when you look at COVID, we’ve been able to get different scientific domains to ramp up very quickly and throw a lot of research and work at these problems relatively quickly. Hopefully these teams and all these great scientists that have been working on this problem can be able to pivot and work on some of the other things that we thought we couldn’t fix or solve previously. |