|
Interview by: Makena Binker Cosen (CC ‘21)
Cover illustration by: Arooba Ahmed (CC '23)
The following is a heavily condensed version of the full interview. If you're interested, read more here. What inspired your current COVID-19 research project? During the early days of the pandemic, I felt myself wishing there was something I could do to help. Then, I started thinking, maybe there’s a way we can apply policy or economics to evaluate ongoing responses to coronavirus. Towards the end of March, I noticed that many elective procedures and other in-person visits were being postponed or cancelled for non-COVID patients. That got me thinking about the many indirect effects the pandemic is having on healthcare. Also, people who used to get routine care were avoiding healthcare settings due to fear over potential COVID exposure. Meanwhile, people still need treatment for heart attacks, strokes, and cancer. Overall, there has been a tremendous shock to the healthcare system, for both patients and providers. What are your current project’s research aims?
To specifically study health outcomes among non-COVID patients, we could also use electronic health record data from hospitals. The approval process to access that data can be a bit lengthy. However, once we find a willing partner to provide health record data, analyzing it and developing preliminary results should only take a month or two. The second challenge is methodological. Let’s say we identify some effect on health outcomes for non-COVID patients — how do we know it was caused by a delay in their treatment and not by other factors, such as sudden unemployment or the loss of health insurance? There are many confounding factors that make it tricky to isolate a particular causal relationship. Moving forward, what do you think the broader impacts of the pandemic will be?
insurance coverage. The possibility of another economic downturn, like what is happening now, will challenge employers to reconsider how they structure their benefit packages and their general approach to worker health. If anything, we now see the importance of innovations that employers are testing to encourage improved quality and efficiency of care, and to restructure the way that employee healthcare is delivered and paid for.
0 Comments
meta name="twitter:card" content="summary_large_image">
By: Makena Binker Cosen (CC ‘21)
I was hoping you could start by describing your background as a researcher. Thanks so much for reaching out. I really appreciate this opportunity. I’m an assistant professor of health policy and management at the Mailman School at Columbia. This is my second year now. I first started learning about health economics and health policy when the Affordable Care Act was being debated and passed. At the time, I was actually working in state government as a policy advisor. It was just really interesting to see health policy start to take shape, especially at the state level, thinking about how we are going to implement health insurance exchanges or how these pieces of legislation are going to move forward. I saw the role that academic research plays in policy making first-hand. After I finished my time in the State Senate, I started graduate work at the Wharton School. I did my PhD there in applied economics with a focus on health economics. After that, I did a fellowship at Harvard. I was at Harvard Medical School for two years—that’s when I first started thinking about issues of healthcare payment and delivery. I started doing research looking at alternative and value-based payment models, new models for paying physicians to encourage efficiency and cost-reduction while still maintaining the quality of care. For that reason, I became very interested in Medicare and associated innovation around physician payment. That background built my current research at Columbia prior to COVID. If you think about it, the majority of non-elderly adults in the U.S. receive their health insurance through their place of work. In the U.S., we have a system where we’re very dependent on employers for our health insurance. Within this framework, I feel like employers can really play a large role in shaping the costs and the quality of healthcare that we can get, especially in the case of large employers. For instance, take Silicon Valley. Many companies have these really nice on-campus clinics and gyms. You could basically leave your desk, go get primary care, and then very conveniently be back at your desk within an hour. These employer-based innovative models of care delivery are what I began studying with my PhD dissertation. What does that mean for your outcomes? What does that mean for your spending? What does that mean for your utilization of other types of services? For example, employers like Walmart are now offering low-cost insurance plans for their employees where they get all of their care from one provider group, like Emory Healthcare. Another example would be Walmart negotiating with John Hopkins Hospital and saying, “We’re going to fly any employee, regardless of where they are in the country, to your health system if they need spine surgery, and we’re going to cover their travel costs too.” Employers hope this direct contracting model will lead to better outcomes and cost-savings down the line. Broadly, that's what has been on my research agenda. Then, COVID happened. I started to think, “How can health economics, health policy, and applied economics be used to study some of the things that are going on?” Especially in the early days of the pandemic, I felt myself wishing there was something I could do. Then, I started thinking of what we can do with policy or economics to evaluate what is going on and maybe say something about the current state of government response to the pandemic or what’s happening outside of the numbers of cases and deaths. Great, that brings us up to the next question. What has your transition into COVID research been like? What have you been able to bring to the table and how has that shaped the objectives of your research project right now? Back in mid-March, the first thing that stood out to me about COVID was school closures. With schools closing, a lot of students would not be able to get school lunches, for example. We didn’t know how long this was going to go on for. If school age children are not able to go to school, that interrupts their educational process and ability to get needed nutrition. What will be the lasting impacts on their health, nutrition, chronic condition management, and ability to find a job and remain employed? There are a lot of indirect effects of the pandemic that we will need to pay attention to down the line. After talking with some of the senior faculty in my department, I started thinking that there are a lot of interesting indirect effects within healthcare that we don’t understand. Towards the end of March and the beginning of April, things started to really worsen with COVID, especially in New York City. I read many articles and news clips where people were talking about how a lot of elective procedures are being cancelled and in-person visits are being postponed. People who used to be getting primary care are afraid of going to their offices and being exposed to COVID. This is a sudden shock to demand for healthcare. What might be the consequences of people not being able to get some types of treatments? At first, I thought that maybe these are just elective procedures that can wait, like hip replacements. Then I started seeing articles where patients were saying, “I need an organ transplant. I need a surgery to remove pre-cancerous tissue. I need to go in for regular cancer treatment.” That’s how I started thinking that there was an interesting project to do here that looks at some of the consequences or the potential effects of delayed or forgone care on non-COVID patients. The news will tell you the number of confirmed cases and deaths. Even then, researchers believe those numbers are underestimates. If you think of the full toll of the pandemic, there are a lot of indirect effects that we don’t understand as well. Not just on mental health, the economy, or education, but on how the healthcare system is functioning; on non-COVID patients who also have urgent needs. Heart attack, strokes, and cancer are still happening in the background. That’s where I launched into thinking about the indirect effects on non-COVID patients' outcomes. What are some of the specific questions or themes you are looking at? How do you hope to address them in this project? I envision two main aims. The first aim would be to look at the potential effects of delayed or forgone treatment on non-COVID patients’ short- and long-run health outcomes. For example, two groups I would be interested in studying are cancer and transplant patients. How long does it take them to get their procedures done? How do their outcomes compare to patients who did not have their treatments delayed? COVID is starting to be on the decline in many cities, so a lot of health systems are trying to bring back these procedures. This provides a very interesting setting to study what happens during this delay. The second aim involves studying what is happening to in-person primary care utilization. A study from The Commonwealth Fund finds a large drop in in-person ambulatory care utilization that occurred during COVID, followed by a slight rebound. As the months progress, how much of a rebound will we see? Will things get back to pre-COVID levels? How long will it take for people to start using in-person care again? It seems that it’s definitely ramping back up and people are going back to see their physicians and other types of clinicians. On a similar note, there are New York Times and ProPublica articles where people are saying that there are not that many heart attacks, strokes, or appendicitis cases coming into hospitals anymore. That doesn’t make sense. Those types of conditions are still happening. It’s just strange that they wouldn’t be showing up in the hospital. A lot of these articles claim anecdotal evidence, but there is no supporting data available yet. That’s one thing I’m very interested in trying to figure out. Can we find data that shows what’s happening with these patients? Are people with heart attack, stroke, and appendicitis just not going to the hospital? Are they dying at home? Are they waiting for their condition to be very serious? And if they wait until their appendix has ruptured already and now have a very complicated and severe condition, would it have been more easily handled if they got treatment earlier? That’s a very good point. It’s definitely something I’ve also wondered with all of these articles coming out. It’s really good to see someone trying to find those answers. You’ve described interest in several stages of the pandemic, including pre-pandemic times, its early beginnings, months in, and — what will hopefully come soon — a post-pandemic world. I’m curious to know, what general timeline do you expect for this project? That’s a good question. Right now, I’m in the process of working with a Master of Public Health student in the Mailman School to figure out what data sources are available. This has been one of the biggest challenges. The pandemic and its effects are moving so quickly, and they keep evolving. There is a lag between when data is collected and when it becomes available to researchers. To look at health outcomes among some of these non-COVID patients, we could use electronic health record data from hospitals. The only issue is the approval process for getting that data can be a bit lengthy. However, once we are able to find a willing partner to provide health record data, analyzing it and getting preliminary results may only take a month or two. At least right now, we are not going to apply really fancy econometric methodology to do this work. A lot of the initial work, and some of what will be the most important work, is just looking at raw trends in the data. For example, what’s going on with utilization of care? Another component of my planned research, and the New York Times has been talking about this, is examining the issue of excess mortality. For example, you could use historical data to generate a projection of deaths in March 2020 for New York City. It turns out that the actual number of deaths is much higher than the estimated number of deaths. Roughly 80% of these excess deaths are attributable to COVID cases or probable COVID cases. I would like to figure out what is going on with the other 20% of excess deaths that are not attributable to COVID. Again, it has been tough to find data for that, but the CDC is one potential source. There’s also some data available through the NYC Department of Health and Mental Hygiene. Now, I’m trying to figure out what data is publicly available that we can get and use right away. After we figure that out, within one or two months, it’s possible to start getting some preliminary findings. That would be great. You mentioned getting data will be a challenge, which would be a huge hurdle for a project that relies on processing data. Are there any other challenges or caveats you expect at the moment? Yes. The first challenge is any lag in collecting and getting the data. The CDC has done a great job compiling data and the New York Times has actually been utilizing a lot of it for their interactive analyses. If we want to get actionable findings out there quickly, the best bet will be to use publicly available datasets like those from the CDC. The New York Times or FiveThirtyEight could help with data also. The second major challenge will be on the methodological end. How do you isolate the effect of COVID? Say you find some effect on health outcomes for non-COVID patients, how do you know that is because of delayed or foregone treatment and not because they lost their job or health insurance or something else going on in the healthcare system? It is going to be difficult to say that delaying treatment or missing this appointment led to this result, because there is so much going on in terms of mental health issues, or the economy, or losing your job or your partner losing their job. There are all these other confounding factors that could be taking place. It is going to be tricky to isolate a particular causal relationship. I appreciate how deeply you’ve been thinking about all of this. You’ve outlined some areas in which healthcare has been impacted by the pandemic. What is your perspective on the future regarding your research and the broader impacts of the pandemic? As for my research interests, these projects that just came onto my radar during the pandemic are really interesting, but they are very time-sensitive. I would like to work on them and try to get these findings out quickly. After that, I would like to pivot back to some of my core interests, such as innovation in healthcare delivery and payment. There is going to be an interesting opportunity to see how employers are responding to the pandemic. There have been so many lost jobs. We’ve seen wide variation in terms of the impact on employers. Employers with employees who can work remotely may have been less impacted than companies or industries where people have to go in to work. Moving forward, employers will need to think a lot about investing in worker health. How do you protect your workforce? How do you prepare for these types of situations where health insurance or healthcare might be disrupted? Hopefully, there’s not another pandemic, but this will challenge employers to think, “We need to be careful of these types of situations where there could be a devastating impact on healthcare and health insurance for employees. So, how do we restructure our benefits and our approach to worker health?” That’s going to be something that I’m very interested in keeping up with. In a post-pandemic world, what types of investments are employers going to make? As for the broader impacts of the pandemic, two thoughts. First, it’s interesting that we are seeing a rebound in outpatient visits, as shown in recent Commonwealth Fund research. I think it was in March that ambulatory care visits dropped by 60%, compared to pre-COVID levels. Now, they’ve rebounded slightly, but volume is still about 30% below pre-pandemic levels. It will be really interesting to see how long it takes before people start to go back to interacting with healthcare providers on a regular basis. It may take some time, but I do think eventually we will get back to a place where people feel comfortable doing so. People need to see their clinicians and need to get care. Second, COVID has been a big shock to health systems’ finances. There are a lot of hospitals that are reliant on elective procedures for revenue. When those got canceled or postponed, that was a big shock to their finances. Now that visits are starting to rebound, the big question to consider is what are hospitals’ finances going to look like? Are some going to have to close? Are some going to be okay? Overall, I think the pandemic is going to play a very big role in the 2020 election. I’m very interested to see how the candidates talk about reform in the U.S. healthcare system in light of what happened with COVID. Maybe, we’ll see more momentum towards expanding affordable health insurance coverage options for Americans. It is critical for people to have adequate and stable health insurance coverage, in case something like this happens again. Most definitely. Moving forward, do you think innovation in terms of employer-based health care will be stifled or transitioned to a different model? In the United States, we have a system where, in general, adults under the age of 65 are largely dependent on their employers for insurance coverage. With the pandemic, a lot of people who lost their jobs also lost their insurance coverage. I think that this is going to come up in future debates. Do we need to rethink this system where insurance is so heavily tied to the place of work and to your employer? What happens if you lose your job and you lose access to health insurance or healthcare services? I also think that this pandemic will actually encourage employers to invest more heavily in worker health. Employers are seeing how important it is to have a healthy workforce and to have a workforce where people are insured and covered just in case there are any shocks to the economy, like what is happening now. If anything, we now see the importance of innovations that employers are testing to encourage improved quality and efficiency of care, and to restructure the way that employee healthcare is delivered and paid for. I think that these types of innovations will actually pick up momentum in upcoming years. Under this model of employer-based healthcare, where do self-employed individuals stand? That’s a good question. The focus is often on people who are employed by mid-to-large-sized corporations. Those corporations have the resources and ability to pull together people to buy insurance plans. It’s much trickier and more expensive for people who are self-employed. I think that’s going to be a major issue coming up in the 2020 election, especially in light of what has been happening with the pandemic. Do we have robust enough options for self-employed individuals to buy affordable health insurance coverage? The Affordable Care Act tried to address this through the creation of health insurance exchanges, but there is still more work to do. What are the mechanisms that we need to have in place to make health insurance coverage more affordable for self-employed or unemployed individuals? It’s going to require broader healthcare reform to address those issues. Wrapping up, do you have any recommendations for patients who are currently facing delays or cancellations for non-COVID-related procedures and treatments? I haven’t discussed this directly with any patients, though I have heard cases and read articles about it, such as those on ABC News and ProPublica. Health systems are beginning to ramp up in-person visits and procedures again. Many providers have responded well and adjusted their operations to ensure that the risk of COVID exposure is low, so patients should feel safe to receive in-person care. On another note, while it’s tough right now, maybe there is a possibility that Columbia could collaborate with one of the major health systems in New York, like NewYork–Presbyterian, Mount Sinai or Northwell, to push out a survey or interview patients to see, “Has this issue affected you? Are you afraid to seek care? Have you had your treatment delayed? How do you feel about that?” I think that these results would be really fascinating. It really would be. Is there anything else you would like to add? Right now, things are evolving so quickly with the pandemic. There is concern about what is going to happen in terms of re-opening and if we will see flare-ups of COVID again in certain areas. We are really seeing the power of data in all of this. That includes electronic health record data, GPS coordinate data, or even data that Google or Apple could potentially collect. We are fortunate to live in an era with robust data collection capabilities. There is so much power analyzing these large datasets to uncover any relationships that might exist between, say, containment policies or other strategies and outcomes that are of interest to the general public, like access to care, cost of care, or COVID-related outcomes. Especially with the Columbia Science Review getting the word out about what research is going on, it will be interesting to use those analyses to see what did or didn’t work in terms of the responses to coronavirus.
By: Christina Lee (CC ‘21)
Cover illustration by: Ara Uhr (CC '23)
The following is a heavily condensed version of the full interview. If you're interested, read more here. What types of projects has your lab done in the past? My research has been focused on using embedded platforms, such as the smartphone, combined with data analytics methods, such as machine learning, to solve real-life problems. I think that’s something that has carried over with me when I joined Columbia five years ago. My lab is trying to work on research that tackles real-life problems. For example, in the pedestrian safety project, we developed technology that could enable pedestrians to better sense the world around them. They can be alerted in advance when a vehicle is on a collision trajectory. A lot of our other projects also have similar real-world motivations.
When the COVID-19 situation started, the hospital that my wife works in was facing a lot of shortages in PPE and personnel. During the check-in process, they needed to take the temperatures of patients. Since they had a lot of patients coming in, the check-in process was very slow, so they needed a better solution to screen patients. This project would potentially address this need.
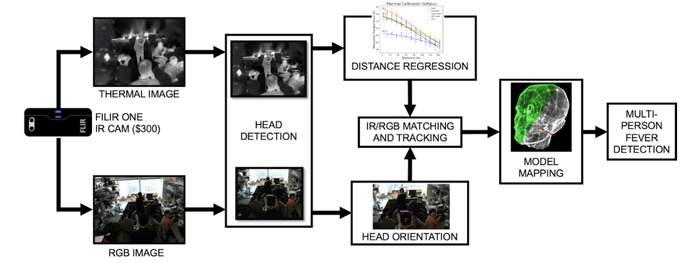
Data Processing Pipeline. Image courtesy of http://icsl.ee.columbia.edu/FeverScreening/
How has your progress been, and have you encountered any setbacks? So there are some technical challenges we are addressing right now: 1. Accuracy of an affordable thermal imager: We are trying to find a way to improve the accuracy of thermal images taken using a low-cost thermal imager. We developed a data-processing pipeline where we can first create a 3D model of every single person in the frame. Once we have a 3D model of every person, including his or her head, we can then map the images that we’ve taken so that instead of relying on a single image, we can add more images to the 3D model of the human head with the correct orientations. Since a person is not always looking at the thermal imager, the traditional approach is not going to get a very consistent and accurate shot of the face. With our approach, regardless of which side of the face is facing the camera, we can conform it to the 3D model of the head so we can continuously improve screening accuracy with the data that is incoming in. 2. Calibrating the thermal imager: Different distances, humidities, and temperatures can all affect how pixel values translate to actual skin temperatures. This is something that requires time and many experiments to obtain calibration data, so that’s what we’re working on now. We have a working prototype, but we’re still trying to improve it. What do you think the public should know about the timeline of your research? What is your perspective on the future of your research and its impact on COVID-19?
I really hope that this will have a long-lasting impact on the healthcare industry and many other places that can use a system that provides continuous detection of fever within a population. So maybe in the future, schools, cruise ships, buses, or subways can use this, and I really feel like this could be a game-changer.
By: Makena Binker Cosen (CC ‘21)
Let’s start with your background as a researcher. How far back would you like to go? As far as we need to go to understand what fields influences the way you view research today! My background begins with nutrition. I have a PhD in Nutrition from McGill University and my research focuses on sleep as a causal risk factor for obesity and cardiovascular disease. I started my research career mostly interested in diet and life-style behaviors, and how those could influence cardiometabolic risk factors. Then I got pulled into the sleep field when there was an increased awareness of a relationship between sleep duration and obesity. The field was trying to figure out why that would be the case. How could sleep influence energy balance? At that time, where I was, sleep researchers wanted to get someone who had expertise on the measurement of energy balance to be able to help them respond to a call for grant applications by the NIH. I knew nothing about sleep. However, I was very interested in how lifestyle could impact energy balance regulation and was very open to the idea of bringing my expertise to this group and helping them assess energy balance in relation to sleep duration. Then, the grant didn’t get funded. I moved away from that institution, back to Columbia, where I had done my post-doctoral fellowship. I reapplied and kept applying for this grant to really assess whether sleep was a causal factor in the regulation of energy balance and a causal factor in the development of obesity… and the grant got funded! From there on, I became a sleep researcher. It was very fascinating. Also, a lot of the researchers in the field of sleep are psychologists or medical doctors—people without a nutrition background trying to get at how sleep influences aspects of life that are also influenced by food intake and physical activity level. So, I’m very aware of how intertwined those two fields are. A lot of the hormones that regulate sleep also regulate appetite and food intake. Therefore, if you’re trying to isolate the influence of sleep on metabolic risk factors or obesity, for example, we also have to take into account what is going on with the food intake and physical activity level. That’s where my research is different from what others do. Now, I’ve really begun to think about sleep and diet as having a bi-directional relationship and really wanting to figure out what we can do in the diet space and nutritional space to influence sleep and help people sleep better. Maybe doing that will help them achieve better diets and better life-style practices. That’s absolutely fascinating. You have a lot of experience integrating your previous research into new fields and venturing forward with interdisciplinary projects, which is very impressive. I always tell my trainees that you have to keep an open mind; not to go into their careers with a very narrow focus. You never know where research will take you. When these sleep researchers came to my department and asked for someone to help them measure energy balance, we were two investigators in that space and I was very junior. The other investigator was much more senior. At the end of the meeting they told me, “I’m not interested in sleep. If you want it, go for it. It’s all yours.” I didn’t know anything about sleep at that time, but I thought, “it’s just a different way of applying my knowledge” and I think that can be very interesting. That opened up a lot of doors for me and really helped me find my niche, so to speak. It sounds like your flexibility opened a lot of doors, but it also brought your expertise to where it was truly needed: sleep research needed a nutrition perspective and you really brought that through. In relation to your current research, how can we expect the COVID-19 pandemic to influence the way people sleep? There could be many different ways that the pandemic could influence sleep. Sleep timing and meal timing is very dependent on your personality and personal preferences — your chronotype, as we call it. In general, anxiety and depression brought on by this pandemic could really adversely influence sleep. On the one hand, if individuals are worried, it keeps them up at night; they are not able to fall asleep readily. On the other, it might make them more depressed, and depression is associated with longer sleep. What I always say helps with sleep is waking up at a regular time, going to bed at a regular time, and getting sunlight during the day. I can imagine in the city that it might be difficult for some people to really get that dose of sunshine when they wake up in the morning, if they’re living in tight quarters and are not able to get outside. So that’s also something that can impact their circadian rhythms and have a negative influence on their sleep. Working remotely could also have various benefits considering that people aren’t commuting. If they are not spending an hour or two commuting, they can sleep in a little longer and maybe get adequate sleep during the week, just as they may get adequate sleep on the weekends. Now more than ever, the general public is aware of the relationship between sleep and mental health. How do your earlier recommendations, i.e. waking up and going to bed at a regular time and getting sunlight, contribute not only to our mental health but to staying healthy during the pandemic? That is to say, how does sleep influence our risk of having COVID-19? There have been studies that look at your susceptibility to viral infections based on sleep duration. If you’re not sleeping enough, you are sleep restricted and at a higher risk of catching a viral infection or experiencing related symptoms. The issue is that your immune system is suppressed when you don’t get adequate sleep. That’s actually something that we’re trying to look at right now with our research. Over the years, we’ve screened almost 250 people with wrist actigraphy, so we have objective sleep data from all of these people prior to the pandemic. We want to contact these people again and see what proportion were infected by the virus. How many had symptoms? How many were treated? What were their outcomes? Ultimately, the goal is to see if there is a relationship between the sleep we measured prior to the pandemic and the symptoms during the pandemic. How has your progress been in this project so far? Have there been any setbacks? We’ve been applying to the Institutional Review Board (IRB). We’re creating a list of all participants to be able to call them up. I imagine the IRB is very busy right now. Everyone must be trying to push their projects through. The IRB is very responsive, actually. We’ve been able to start a new project, which has been great. We’re conducting a well-being study that we decided to take completely online when the pandemic started. We were right about to get it started bringing participants in for counseling with a PhD student of mine when the pandemic hit. So we were no longer allowed to have in-person visits at the Medical Center and we thought this might be a good opportunity for us to test our ability to do counseling online, to conduct research with telemedicine and to see how that goes. We have to try to make the best out of these situations that are thrown at us. It’s interesting that you bring up telemedicine. It seems like this is going to be a trial period to see how far we can take it, how we can improve it and how we can integrate it to previous research and healthcare models. What’s your perspective on the future, regarding both your own future and the broader impacts of COVID-19 upon the scientific community? I think it’s definitely going to be more challenging for researchers like me who do clinical research. We’re used to very stringent protocols where we’re bringing people into the clinical center to make sure that we’re verifying everything objectively; that all of our measures are taken on site. Now we have to explore different ways of conducting research that are not necessarily bringing people into the Medical Center. We’ve had studies where people come in every single week for us to verify their sleep. Maybe they don’t need to come in every single week. The battery life on the monitors we use to measure sleep lasts up to 3 weeks. Perhaps we can space out our visits to reduce on-site testing. We can combine this with virtual visits to verify questionnaires. Those are things we’re thinking of doing now. I imagine it might be complicated to conduct research without bringing people into the Medical Center. How do you set up and monitor controls to give your results validity? That will be an interesting challenge. So, yes and no. In one way, for us, it removes a little bit of control from the study. At the same time, it may be very helpful for recruitment. How many people can make the trip up to the Medical Center if they’re working, for example, in Brooklyn or Queens? How many people can come to the Medical Center on a weekly basis? Maybe that would allow more people to participate in our research because they don’t have to have these commitments. That’s an excellent point. With what we know right now, what do you expect the timeline of your COVID-related research to be like now that you’re in the application process? I assume we will be able to get it started really soon. We haven’t really had much waiting time between reviews with IRB. Data collection will probably take a couple of months since everything will be virtual visits on the phone or online by questionnaire. From the description on Columbia’s Research website, I understand that it’s going to focus mostly on sleep. Is there anything you’re going to bring in from the nutrition side? We have a questionnaire that asks if you’ve had a change in weight or diet over the pandemic, but nothing in terms of actual food questionnaires. We want to keep it simple. The questionnaires are quite extensive. It’s hard. You have to be selective I imagine with the questions you ask so there aren’t too many. You need to achieve a right balance between critical information and participant burden. Wrapping up, is there anything you think people should know right now, any final thoughts on sleep, nutrition, or both? I think people should try to keep rhythms as stable as possible — a stable bedtime and a stable wake time, achieving adequate sleep duration of at least seven hours per night. If possible, it’s great to get a little bit of sunshine outside. When you’re indoors all the time close to your kitchen, close to your fridge, it’s very easy to just go and grab something to eat in between meals. If you were in an office, you really wouldn’t have access to food as readily; you wouldn’t have the leisure to eat at any time. So, trying to keep those stable patterns of food intake, so as not to be over indulging. Also to keep in mind that we are not really commuting anywhere. I just walk from my bedroom to my home office. I used to ride my bicycle to the office, thirty minutes each way. You have to find new ways of being physically active to compensate for that. 
Cover illustration by: Sahra Denner (CC '21)
Interview by: Makena Binker Cosen (CC ‘21)
The following is a heavily condensed version of the full interview. If you're interested, read more here. Can you explain your interdisciplinary background as a sleep researcher? My background begins with nutrition. I have a PhD in Nutrition from McGill University and my research focuses on sleep as a causal risk factor for obesity and cardiovascular disease. I got pulled into the sleep field when there was an increased awareness of a relationship between sleep duration and obesity, with the key question: how do sleep and personal lifestyle influence energy balance?
So what’s the connection between sleep and this pandemic? There could be many different ways that the pandemic influences sleep. Sleep timing and meal timing is very dependent on your personality and personal preferences (a.k.a. your chronotype). In general, anxiety and depression brought on by this pandemic could really adversely influence sleep. On the one hand, if individuals are worried, it keeps them up at night; they are not able to fall asleep readily. On the other, it might make them more depressed, and depression is associated with longer sleep. What I always say helps with sleep is waking up at a regular time, going to bed at a regular time, and getting sunlight during the day.
Over the years, we’ve screened almost 250 people using wrist actigraphy (a special body sensor), so we have objective sleep data from all of these people prior to the pandemic. We want to contact these people again and see how life has changed for those infected by the virus. How many had symptoms? Were they treated? What were their outcomes? Ultimately, the goal is to see if there is a relationship between the sleep we measured prior to the pandemic and the symptoms during the pandemic.
What’s your perspective on the future of your research & beyond? It’s definitely going to be more challenging for clinical researchers like me. We’re used to stringent protocols where we’re bringing people into the clinical center to make sure that we’re verifying everything objectively; all of our measures are taken on site. Now we have to explore different ways of conducting research that are not necessarily bringing people into the Medical Center. We’ve had studies where people come in every single week for us to verify their sleep. However, the battery life on the monitors we use to measure sleep lasts up to 3 weeks, so we can space out our visits to reduce on-site testing. We can combine this with virtual visits to verify questionnaires. In one way, it removes a little bit of control we have over the study. But at the same time, it may be very helpful for recruitment. How many people can make the trip up to our Medical Center every week if they’re working in Brooklyn or Queens? Maybe this will allow more people to participate in our research because they don’t have to have these commitments. Any final thoughts on sleep/nutrition we should know about?
something to eat in between meals. If you were in an office, you really wouldn’t have access to food as readily. So, trying to keep those stable patterns of food intake, so as not to be over indulging.
Finally, watch your physical activity. We are not really commuting anymore. I, for one, used to ride my bicycle to the office, thirty minutes each way. We have to find new ways of being physically active to compensate for that. Interview Highlights: “The Cloud” & Living Through COVID-19 Infection with J. Thomas Vaughan Jr.5/28/2020 
Cover illustration by: Zoe Chan (CC '22)
Interview by: Hannah Lin (CC '23)
The following is a heavily condensed version of the full interview. If you're interested, read more here. Can you describe your COVID-19 research? We have a collaboration of about 30 people—physicians, staff, faculty—across Columbia. The title of our research is COVID-19 Longitudinal Multi-ethnic Bioimaging Assessment of Cardiovascular Sequelae. Now that’s a mouthful—obviously the physicians thought that one up [laughs]. They worked hard to come up with an acronym. If you use the right letters in the right sequence, that adds up to COLUMBIA CARDS registry.
We’ll image and compare the differences between 2 cohorts: one healthy normal group and one COVID antibody positive group. We’ll use a number of different techniques to characterize myocarditis: a viral disease of the heart and resultant heart ailments.
2. To assess the effect on myocardial function of COVID-19 infection in a multi-ethnic spectrum of convalescent patients and to relate functional features to the patient important outcomes. In other words, we’re looking at a broad spectrum of people from different ethnic groups, walks of life, races. New York is great for these kinds of populations.
Cloud Platform. Medical imaging is 90% of the data amassed from a hospital or clinic, so it requires huge amounts of archival space.
So we really have to look to the cloud, to the future, for archiving medical image data and also for looking at that data rapidly and broadly to correlate to symptoms or anything else. Data’s the oil, the gold, the currency that so many people are beginning to trade and, frankly, makes a lot more sense than dollars and gold bars—it’s more useful. It’s knowledge. The more data we acquire from our huge, diverse patient population, the more information we have to ask big questions about certain symptoms, therapies, or differences between racial or ethnic groups, genders, or ages. Are you still keeping prior projects going?
You’ve had COVID-19 yourself. Can you talk about that experience?
So I knew I was going to get sick from something then. But at the time, frankly, it was so early—February 14th—that I thought it was a cold or flu. You know, this was back when everybody was calling this the “Democratic hoax.” Clearly, it was already alive and well in New York before February 14th; I’m proof of that.
I got home Monday night, and Tuesday morning I woke up with all the characteristic symptoms: headache, a very nonproductive dry cough, all the stomach ailments. It just felt like I’d been run over by a bus; my whole body ached. I was just thinking it was a nasty case of the flu the whole time. Everybody’s affected in different ways; to me, coughing was the worst part because I couldn’t go to sleep at night, my chest and diaphragm ached everytime I coughed, it was just painful. So I stayed doped up on ibuprofen, aspirin, everything else. There was some rumor going around for a while to “not take ibuprofen when you have COVID, because everybody that dies with COVID is full of ibuprofen” like there was some correlation. I’m like, the correlation is that if you’re dying of COVID, you need pain relief [laughs].
Unfortunately, as you see, especially in our own country, this cooperation rapidly devolved and (I’m happy to be on public record for this) because of our lousy leadership, we see an example of the human tragedy that bad leadership, a lack of coordinated government response, and a lack of international collaboration in goodwill can cause. I think we’ll be able to look back at COVID collectively and learn very important lessons across the broad spectrum of what to do and what not to do. I hope we will learn.
By: Hannah Lin (CC'23)
Could you talk a bit about your background? I am an epidemiologist with a background in emergency medical services. I’ve worked in various places—hospitals, communities, morgues. That’s where I got a start thinking about epidemiology. Those are what sparked my interest in population data and epidemiology and the power of these to make positive change for large groups of people. Could you describe your COVID-19 research at the moment? Most of my interests are in trauma and injury— people getting in car crashes, people getting shot with firearms. Some of my work via emergency medical systems has dealt with mass events—responding to disasters, whether they be from epidemics, natural disasters such as floods or earthquakes, or things like mass shootings or bombings. So I have a history doing that. For COVID, a pandemic is yet another form of excessive demand, a form of illness on a large scale. So I started applying what I did with hospitals and healthcare systems to the pandemic by looking at it from a number of different perspectives. One of those perspectives is just the sheer volume and whether we have the right healthcare resources to respond to the volume of cases. The other is the geography of it all—where the greatest risks are, not just simply calculating the risks regardless of place-based disparities. How has your progress been? We have the pre-print publication, and you’re talking to me on a day when I’m working on the peer review revision of that same publication for other scientists to look at. Peer review is when scientists send things out to their fellow scientists—epidemiologists, in this case, and we also have public health scientists looking at this. This is a publication looking at counties across the US and their COVID-19 case forecasts over 6-week windows going into the future to look at which counties are at greatest risk of experiencing high levels of COVID-19. It also looks at matching the demand by patients who are seriously ill with the supply of medical resources in counties across the US. As you can imagine, there are different levels of access to hospitals by county in the US. It varies greatly. Basically, the work is trying to predict which counties are at greatest risk of having their demand of COVID-19 patients exceed the supply of hospital resources, especially critical care. We have the mapping on our websites—it’s always dynamic, it gets updated every Monday morning with the newest figures: https://tinyurl.com/beh-columbia-maps. We also have another website that our programmers made, predicting for every county in the US, looking at the curves for the COVID-19 cases in those counties: https://cuepi.shinyapps.io/COVID-19/. Have you faced any setbacks in gathering these data and making these projections? I’ve been doing this for quite some time, thinking about the population-level surge of illnesses and injuries. The earliest work I did for this was the Oklahoma City bombing and then 9/11. For the Oklahoma City bombing, I was working at the federal government and we had a response to analyze the situation, the people who were injured, and how they were distributed to the hospitals in the surrounding Oklahoma City area. That was a relatively small event, actually, in the grand scheme. The federal government invested a little bit in solutions, but not overwhelmingly. And then 9/11 happened, and there was vast investment in all manner of different things related to disaster response, not just mass casualty trauma, which is a high volume of trauma—like what happened on September 11th—but there was also concern about bioterrorism. So that spilled over into things like what we were going to do if someone weaponized smallpox or released anthrax over a city. There was a lot of resource investment in response, data gathering, modeling, and so forth that then suddenly went away because there were no events in the interim. I think that was a bad decision, and what’s happened is that now, the challenge for us in building these models is that the pandemic caught us by surprise and we at Columbia University and various other universities have had to re-energize past work and pick up the slack. Now, I will say there are people who have been carrying this and doing this all the way through, so kudos to them; I think it’s fantastic that they’ve done that, but they’ve done it with limited resources. Mostly, all this response modeling—whether it’s the health system, testing and tracing, or the demand of the cases themselves—we’ve had to redo it, in some cases from scratch. The federal government and state governments have been supportive, but it’s taken them a little bit of time to get their response systems up and running again, to be honest with you. Some people would argue it’s taken too much time—there are lives that have been lost in the time it’s taken for policymakers in general to get on board with all this. So the data we’ve been gathering have been available to us very freely. We did have some challenges early on in finding the data especially for every hospital in the US—these data are not in a good, publicly available, centralized place. They were in a lot of different databases around the nation. We had a large team of people who took the date and pieced them together to make something serviceable so that we could advise the coronavirus task force, advise the CDC, advise the US Army Corps of Engineers, advise states and counties, in terms of where they should create the next hospital beds. Many different agencies and action-oriented individuals used the data that we created. So you’ve reached every hospital in the US? We have data on every hospital in the US, yes. Almost 6000 of them. Wow, that’s very impressive. So you talked about forecasting in 6 week windows--what is the general timeline of your research, and where is it going in the future? There’s a research component of this in building a model that can then be used going forward into the future. And it does function in 6 week increments, but also in daily increments—every day over those 6 weeks. We’re in the process of not just looking forward and building a model that will continue to function to make these predictions, but also looking back and seeing how well our model has been doing. That’s what I’m in the process of doing today—looking at that model and its accuracy because we want to know if there were overpredictions or underpredictions, over-responses or under-responses. Of course, we don’t want an under-response when large populations of people are at risk—we don’t want to under-allocate resources because people die in those situations. But something that folks might not understand is that over-response is also very dangerous. Allocating more resources than you need is very dangerous because those resources could be sent somewhere else instead of waiting around and not being used. So this model is really an attempt to balance appropriate resource allocation, what we call optimal resource allocation, using various math models. Is your team still keeping prior projects going even while you focus on COVID-19 right now? Yes, for sure. I actually run Columbia’s CDC—Centers for Disease Control—funded injury science and prevention center. We work on all manner of different things, from mass shootings to car crashes and falls. We just had a huge conference last week. There’s been a pent-up desire to have a national conference on injury prevention, especially in the context of the pandemic. A lot of discussions were had, ranging from domestic violence and child abuse on up to suicide. This was all in the purview of the CDC-funded center. We have this conference annually and we typically have it as a regional conference, where people come from New York, New Jersey, and Connecticut come (that’s our regional responsibility on behalf of the CDC), but this year, since we couldn’t hold it in person, we opened it up, and word got out. What was usually about 70 people turned out to be 350 people who came from as far as Alaska to join the conference and talk about issues of injury prevention. Our work as epidemiologists is in many areas, not just infectious diseases and injury prevention – Columbia epidemiologists also lead global work in cancer prevention, cardiovascular disease, the opioid crisis, mental health, and other things. All of this functions and continues to move on. In the context of the pandemic, because so much has changed, but also, broadly speaking, we know that these have always been important and we need to continue to face these other challenges as well. On a related point, and maybe this is the most important answer to your question: the social structure of the pandemic and the horrible disparities, the socioeconomic disparities that have been generated by the pandemic are something that I think our epidemiologists have appreciated from the beginning, but I don’t think the nation is appreciating enough. We have folks that have really been working overtime to think about and reduce the health disparities created by this pandemic, whether this be in our prisons or as a result of structural racism that has festered for generations; equally, I would say, to our people who are working to study the actual COVID-19 cases and the disease itself. So I can’t stress that enough. These health disparities that have been generated by the pandemic are a second disaster upon the first that we really need to take note of and do something about. Are there any common misconceptions you’ve heard regarding COVID-19 that you would like to rectify or respond to? Well, this morning I was reading about indecision by universities. I don’t know if that’s a misconception, but indecision about what to do. It’s tough—university leadership, and the public health people who are oftentimes suddenly placed in these positions of leadership in universities around the nation, are really doing some difficult tradeoffs with safety of incoming students and the desire to go back to classes and to teach. So I feel for them making these tradeoffs, and it’s quite a challenge at the same time: decisions need to be made, and folks need to know, at a minimum, the thinking of these impromptu leaders—a little more transparency in the thinking—and what the tradeoffs are that they’re making. Telling people about the details of those tradeoffs, even if there’s not a firm answer at any given moment, I think would be quite helpful. Definitely agree. Last question: I know you already touched on this a bit, but what is your perspective on the future, both regarding your research and the broader impacts of COVID-19? Our research-for-action is going to march on. We have a group, for instance, organized just prior to the pandemic, that has begun studying gun violence in the United States. It brought together 3 dozen Columbia scientists who are interested in studying gun violence who otherwise would not have met. This remains a very important issue for the United States. In some cities and rural areas, it is going to be an issue that is competing or will compete with the pandemic itself. So there are issues like this that we are not just going to abandon in the face of this pandemic. That said, there is a new context to contend with, I think. In terms of where resources are going to go, that context is going to be important to think about for us. It will be important to manage where there are real risks of COVID-19 and future outbreaks, where there aren’t, and where other health issues rise to the top. So we need to think about that and not slow our research on other very, very important health issues in the United States and the world, whether that be the issue of tobacco, which remains very high; the issue of diet and nutrition (food sciences), which also remain very high; climate change and health is another enormously important challenge that we and everyone else in the world continues to face. I would hate to see these things be given a backseat. But we do need to deal with the current issue of the pandemic and get that to a more manageable situation for everyone’s sake.

Cover illustration by: Zoe Chan (CC '22)
Interview by: Hannah Lin (CC '23)
The following is a heavily condensed version of the full interview. If you're interested, read more here. Could you describe your COVID-19 research? Some of my work via emergency medical systems has dealt with mass events—responding to disasters, whether they be from epidemics, natural disasters such as floods or earthquakes, or things like mass shootings or bombings. A pandemic is a form of excessive demand, a form of illness on a large scale.
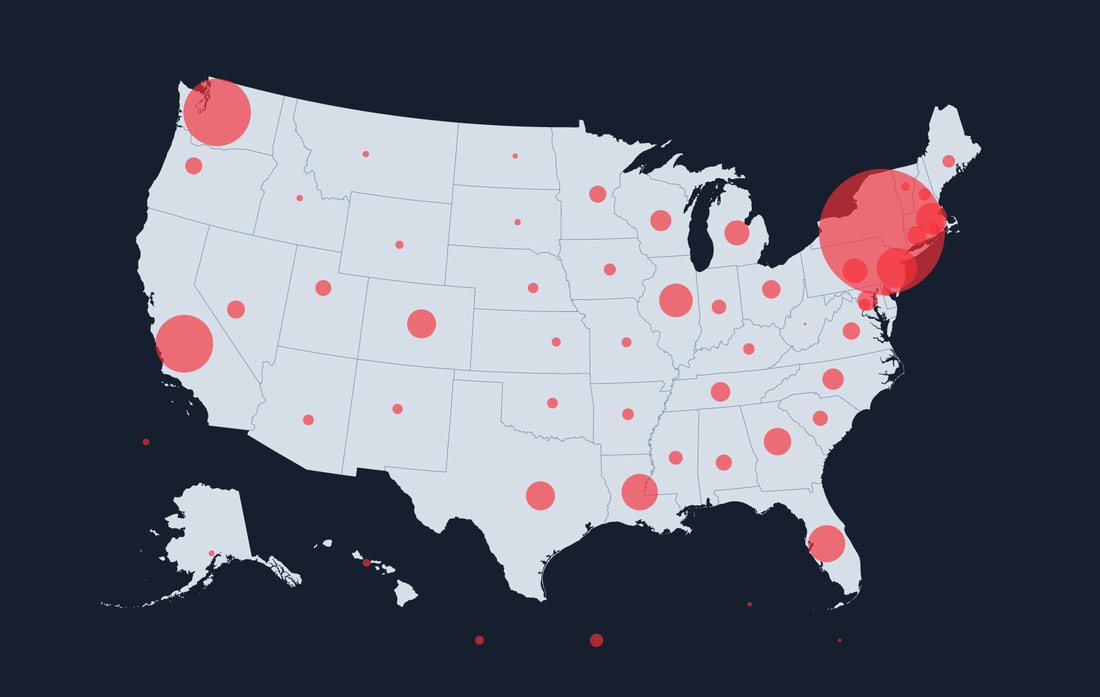
How has your progress been? We have a pre-print publication looking at counties across the US and their COVID-19 case forecasts over 6-week windows going into the future to look at which counties are at greatest risk of experiencing high levels of COVID-19. It also looks at matching the demand by patients who are seriously ill with the supply of medical resources in counties across the US. Basically, the work is trying to predict which counties are at greatest risk of having their demand of COVID-19 patients exceed the supply of hospital resources, especially critical care. We have the mapping on our websites: Have you faced any setbacks thus far? I’ve been doing this for quite some time, thinking about the population-level surge of illnesses and injuries. When 9/11 happened, there was a lot of resource investment in response, data gathering, modeling, and so forth that then suddenly went away because there were no events in the interim. I think that was a bad decision, because now, the challenge for us in building these models is that we at Columbia and various other universities have had to re-energize past work and pick up the slack. Mostly, all this response modeling—whether it’s the health system, testing and tracing, or the demand of the cases themselves—we’ve had to redo it, in some cases from scratch. The federal government and state governments have been supportive, but it’s taken them a little bit of time to get their response systems up and running again, to be honest with you. Some people would argue it’s taken too much time—there are lives that have been lost in the time it’s taken for policymakers in general to get on board with all this.
So you’ve reached every hospital in the US? We have data on every hospital in the US, yes. Almost 6000 of them. Wow, that’s very impressive. What is the general timeline of your research, and where is it going in the future? We’re in the process of not just looking forward and building a model that will continue to function to make these predictions, but also looking back and seeing how well our model has been doing. We want to know if there were overpredictions or underpredictions, over-responses or under-responses. Of course, we don’t want to under-allocate resources because people die in those situations. But something that folks might not understand is that allocating more resources than you need is very dangerous because those resources could be sent somewhere else instead of waiting around and not being used. Is your team still keeping prior projects going? Yes, for sure. I actually run Columbia’s CDC (Centers for Disease Control) funded injury science and prevention center. We just had a huge conference last week. This year, since we couldn’t hold it in person, we opened it up, and word got out. What was usually about 70 people turned out to be 350 people who came from as far as Alaska to join the conference and talk about issues of injury prevention.
would say, to our people who are working to study the actual COVID-19 cases and the disease itself. I can’t stress that enough. These health disparities that have been generated by the pandemic are a second disaster upon the first that we really need to take note of and do something about.
What is your perspective on the future? Our research-for-action is going to march on. We have a group, for instance, organized just prior to the pandemic, that has begun studying gun violence in the United States. This remains a very important issue for the United States. In some cities and rural areas, it is going to be an issue that is competing or will compete with the pandemic itself. We need to make sure not to slow our research on other very, very important health issues in the United States and the world, whether that be the issue of tobacco, diet and nutrition (food sciences), or climate change and health. I would hate to see these things be given a backseat. But we do need to deal with the current issue of the pandemic and get that to a more manageable situation for everyone’s sake. Full Interview: “The Cloud” & Living Through COVID-19 Infection with J. Thomas Vaughan Jr.5/28/2020
By: Hannah Lin (CC '23)
Could you talk a bit about your background? My position here at Columbia is professor of biomedical engineering and radiology. I’m a PhD, not an MD, so I’m a researcher. In that capacity, I’m director of the Columbia Magnetic Resonance Research Center, which spans multiple footprints. The component facilities of that center are located on the main campus with the School of Engineering and Applied Sciences; on the Manhattanville campus in the Zuckerman Mind, Brain, Behavior Institute; on the medical school campus in Radiology; at New York State Psychiatric Institute; and up at the Nathan Kline Institute, also a New York State Psychiatric research institute, in Orangeburg, about 20 miles up the river. So we have MRI systems—we call them MR systems—at those 5 sites. Actually, I shouldn’t leave out one important one: we also have an animal cancer research system at the Cancer Center on the medical school campus. In this capacity, we try to share resources and talent. It’s a construct in coordination and sharing where we share resources for research using the MR tool. I say MR (magnetic resonance) instead of MRI (magnetic resonance imaging) because magnetic resonance imaging is an important subset of our toolkit that everyone is familiar with, but we also have magnetic resonance spectroscopy. It’s a way we can look at biochemistry and metabolism of the living body non-invasively. We also have functional magnetic resonance imaging, which is a way we look at brain activation. We can do all 3 types of imaging with magnetic resonance. A rapidly developing new frontier is just acquiring the biological signals with MR; not even bothering to make images or something that humans can look at and quickly interpret, but just collecting the raw data and searching the new data with the newest machine learning and artificial intelligence approaches to find biomarkers that correlate biochemistry, structure, or function with symptoms or behaviors. Can you describe your COVID-19 research at the moment? I want to be quick to point out that in the context of this center, this COVID research is a collaboration between physicians at the medical center, specifically Andrew Einstein, Nir Uriel, and Marco Di Tullio, and here on the main campus in the School of Engineering and Applied Sciences, Andrew Laine and myself. These are the principals, but we have a collaboration of about 30 people—physicians, staff, faculty—across Columbia. The title of our research is COVID-19 Longitudinal Multi-ethnic Bioimaging Assessment of Cardiovascular Sequelae. Now that’s a mouthful—obviously the physicians thought that one up [laughs]. They worked hard to come up with an acronym. If you use the right letters in the right sequence, that adds up to COLUMBIA CARDS registry. A lot of people think of COVID by its first symptoms, like the acute respiratory distress syndrome (ARDS). So when people have a hard time breathing, they come into the hospital, possibly requiring a ventilator to handle the respiratory problem, which comes from edema in the lungs—swelling in the lungs because they fill up with fluid, water mostly—and the lungs stiffen somewhat. That combination makes it very hard for people to breathe. When the old and the weak in particular get tired of breathing, they have to be helped out by ventilators. We don’t have a cure for this, of course, so the goal is to help somebody to breathe long enough—to stay alive long enough—for their body to create the antibodies to fight the infection. So that’s what we hear about and see mostly in the news, and that’s what we’re first confronted with by most COVID patients in distress. But it turns out that this virus is very idiosyncratic in that it attacks every individual in a different way. In some individual on some day in some way, it attacks basically every organ or tissue. Some of these effects last well after the initial respiratory distress. For example—and most of these are anecdotal observations so far—a lot of recovered patients will walk away with myocarditis, which attenuates your heart function, your ejection fraction. They might have damage to their kidneys, they might have scarring in their lungs, they might have microemboli in their brains or throughout their vascular system. In youth as well—this is what we’re seeing -looks like Kawasaki disease. People are careful not to call it that, but they just say it closely resembles that. In the Columbia-NY Presbyterian Hospital, which is shared with Cornell-Weill, we had such a large volume of patients. We’ve seen, in addition to respiratory distress, symptoms from all of these other ailments to the heart, lung, brain, vascular systems, and other organs as well. These need to be studied—we don’t know anything about this aftermath of COVID that many patients have to live with and continue to recover from, so we need to first understand them before we can come up with therapies to treat them. Specifically, we are in the early stages of putting together a body of research and collecting preliminary data to start applying for grants with the title I mentioned. The first aim is to assess the effect on myocardial tissue structure of COVID-19 infection in a multi-ethnic spectrum of convalescent patients (patients that are recovered) and relate structural features to patient important outcomes. We will do this with MRI and echocardiogram (ultrasound). In fact, we first screen these with ultrasound because it’s a quicker, easier, and cheaper way to triage the people we want to look at. We’ll do these studies in both healthy normal people for control and in recovered patients. They might not have been patients in the formal sense of hospitalization, but they could be like me (I’ve had COVID too), who just tested antibody positive. So we’ll image and compare the differences between 2 cohorts: one healthy normal group and one COVID antibody positive group. We’ll use a number of different MRI, PET (positron emission tomography), and echo techniques to characterize myocardial inflammation: tissue edema, increased interstitial space fibrosis, microvasculature, and ischemia. Myocarditis is a general term for those, and it basically means a viral disease of the heart and resultant heart ailments. The second aim is to assess the effect on myocardial function of COVID-19 infection in a multi-ethnic spectrum of convalescent patients and to relate functional features to the patient important outcomes. In other words, looking at a broad spectrum of people from different ethnic groups, walks of life, races (New York is great for these kinds of populations). And you see in the news all the time where certain ethnic or racial groups are disproportionately affected. Of course, we don’t know the reasons for that yet—it could be socioeconomic, it could be physiological differences—we just don’t know yet. We can’t treat them or correct them until we understand them. So that’s why we’re always using this multi-ethnic spectrum. The third aim is to develop a publicly available image-driven repository of COVID survivors from the unique northern Manhattan population and develop tools for long-term infrastructure sharing and computing support as well as advanced innovative deep learning based analytic tools including metadata, search and curation, labeling of findings, annotation and classification of measured cardiac function, and outcome prediction. According to The New York Times and Google, we’re the first such biomedical imaging lab fully integrated on the Google Cloud Platform. The Cloud platform gives us essentially infinite storage space and on-demand computing. Medical imaging is 90% of the data amassed from a hospital or clinic, so it requires huge amounts of archival space. It outstrips any local servers. So we really have to look to the cloud, to the future, for archiving medical image data and also for looking at that data rapidly and broadly to correlate to symptoms or anything else. To interpret that data, we also need new kinds of cloud-based tools that you hear a lot about in the machine learning or artificial intelligence realm, and Google has some of those tools, while we’ve developed others. So data is the new gold in not just research anymore, but in the economy in general. Data’s the oil, the gold, the currency that so many people are beginning to trade and, frankly, makes a lot more sense than dollars and gold bars—it’s more useful. It’s knowledge. The more data we acquire from our huge, diverse patient population, the more information we have to ask big questions about certain symptoms, therapies, or differences between racial or ethnic groups, genders, or ages. We can ask all these questions if we have enough data to answer them, so we want to create a very large data repository of COVID survivors on a cloud platform. So those are 3 aims of a grant application that we are now beginning to collect preliminary data for to study the aftermath of COVID. Have you faced any setbacks yet, regarding the cloud, the technology you’re using, or the data you’re collecting? Not really. Things have gone quite smoothly. The cloud integration part went really smoothly. We’re operating now on the Google Cloud Platform, and we’ve contracted a cloud integrator, a smaller company named Flywheel—one of the vice presidents is actually one of my former students. With Flywheel and Google, things have gone very smoothly as far as setting up a cloud-based platform, and with a good part of our MR Center, we’re already fully integrated, storing our data and operating on our data. So that part is not a big factor. What we’re waiting through now—and they’re necessary obstacles—is just getting started with new research in the middle of the COVID crisis, because at once, we’re trying to limit the number of investigators in any building or lab at any one time, we’re trying to do only essential studies to limit both the number of people occupying any space at any one time. And then for the people in those environments, trying to protect them, figuring out what kind of masks, gowns, and where to come up with those with resources that are quite limited, how to test people on the front end and which test to use, getting institutional review board approval for these studies, getting seed grants to pursue these studies with, buying enough imaging time to collect the preliminary data we need to submit grant applications. All of these are just standard elements of protocol in getting going on a body of research and that’s what we’re going through now. It’s just what you do to get from A to B. What is the general timeline of your research? I know you said it’s longitudinal, so is it going to be going on for the foreseeable future? Yes. We’re trying to focus on getting this first grant application out, focused on cardiac (heart) ailments because a lot of these patients aren’t dying from respiratory distress, they’re dying from heart attacks. So our first focus is just to look at the heart, but we have to answer the same kinds of questions and look at similar ailments and problems for the other organs in the body. We’re already discussing 2 additional grants in different directions from this one. One would be on the engineering side, setting up a toolkit of more methods and technologies to use to better image the heart, brain, or other organs affected, so there are different ways to stimulate the signal and receive the signal response from an MR system. There are different kinds of technology—we have antenna-like devices that transmit a stimulus signal and receive a signal response from what we call coils. There are new coils that need to be developed to target some of these specific organs, looking for specific markers. Then there are specific protocols—radio frequency, excitation protocols that we use to stimulate signal responses—that we need to program. There are also other methods by which we acquire the data and interpret the data. Setting up the cloud platform, organizing it in the right files and folders, making it HIPAA compliant because all of the public health information we’re collecting has to be hyper-secure, and sharing and securing it the way we want to share and secure it. Just trying to organize this project in the cloud and figuring out how we’re going to manage the massive amounts of data, which we refer to as data curation. And then how we’re going to interpret the data, so specific approaches using machine learning techniques to look for biomarkers in the data that correspond to symptoms that we observe in the lab or clinic. That would be a more engineering intensive grant focused on tools and methods to apply to investigating the aftermath of COVID in recovered patients. Another more clinical direction would be looking at other organs. Not just the disease pathologies themselves, but also how they affect our lives. If we’re looking at the brain for example, we’re seeing a lot of younger patients, some of them not even symptomatic, having essentially mini strokes. We look at their brains where there are what we call microemboli, which basically means mini strokes throughout their cerebrum that can affect those afflicted in very subtle ways, like behavioral changes. People are concerned—we can definitely see, can measure the mini strokes, and strokes in the wrong place in the wrong way at the wrong time to the wrong extent can affect behavior, memory, or other body functions. So all these things have to be investigated. We have the imaging tools—MR is a wonderful one-stop-shop imaging tool in that you can look at structure, like anatomy, to high degrees of resolution; you can look at biochemistry and metabolism; you can look at physiology and function. All of this can be done non-invasively, without interrupting the system in any way on an outpatient basis. We can study large populations of people easily this way, which we plan to do. We’ll start with the heart, and that will help us gain experience in looking at recovered COVID patients. From that experience, we’ll know better what tools we need to develop, both hardware and software, and that will lead to studying other organs. The next organ we will be studying will be the brain. In quick succession we’ll look at the lungs. Graham Barr, a very famous investigator here, has a huge grant for lung studies. We’ve got the tools to look carefully at the ravages that COVID is doing to our bodies. As I said, COVID affects everybody in so many different ways, so it’ll take a lot of work to get our hands and brains around this. So as you focus on this new COVID-19 research, are you still keeping prior projects going? Oh yeah. For MR research, we’ve had to handle this period in 2 ways. We have a lot of research going; across the Columbia campus we’ve got over 120 investigators using MRI or MR in some capacity, supported with over 120 million dollars in NIH funding. Most bodies of research had to be paused just to limit the number of people coming and going in all the buildings and labs on campus. But there are a few studies deemed essential, such as longitudinal studies of disease progression. For example, one of them is Alzheimer’s and another is Huntington’s disease. Unfortunately, we can’t pause the progression of these diseases in patients; therefore, we can’t pause the experiments, imaging them to document their disease progressions. The Institutional Review Board for Columbia decides what research does get done and how it gets done. We’ve continued a small number of deemed essential studies through the COVID period carefully, regulating the number of people involved and how they’re escorted in and out of the facilities, masks, sanitizing all the surfaces before and after. So yes, we have continued a small amount of our “essential” research, but we've had to attenuate most of it, or just put it on pause, anything that we could. You said you had COVID-19. Can you talk about that experience? Sure. I was actually one of the earliest cases. I remember very specifically where, when, and how I got it. I was sitting on a plane out of LaGuardia, back in the cheap section, where everyone has to sit on everybody’s laps. I thought I was going to get lucky on a very crowded plane—I had a seat empty next to me, but at the last minute, this guy got on who had a very characteristic dry hack. And the whole time he was sitting there, he was coughing and had to keep getting up to go use the bathroom and having me hold his coffee cup. So I knew I was going to get sick from something then. But at the time, frankly, it was so early—February 14th—that I thought it was a cold or flu. You know, this was back when everybody was calling this the “Democratic hoax.” Clearly, it was already alive and well in New York before February 14th; I’m proof of that. I was going to a weekend of collaboration at the University of Minnesota, and that went fine. I got home Monday night, and Tuesday morning I woke up with all the characteristic symptoms: headache, a very nonproductive dry cough, all the stomach ailments. It just felt like I’d been run over by a bus, my whole body ached. I was just thinking it was a nasty case of the flu the whole time. And I still should have stayed home, but very foolishly, I had all this super important work that needed to get done in my mind, even though nothing is as important as people’s health, so I’m faulting myself, necessarily. I continued to try to work through this thing, but I just felt awful. Coughing was the worst part. Everybody’s affected in different ways; to me, coughing was the worst part because I couldn’t go to sleep at night, my chest and diaphragm ached everytime I coughed, it was just painful. So I stayed doped up on ibuprofen, aspirin, everything else. There was some rumor going around for a while to “not take ibuprofen when you have COVID, because everybody that dies with COVID is full of ibuprofen” like there was some correlation. I’m like, the correlation is that if you’re dying of COVID, you need pain relief [laughs]. Anyway, it was pretty bad, and I felt just rotten for about 10 days. My wife, also a professor at Columbia, caught it from me very quickly. Strangely, my daughter living with us, who’s a graduate student at Columbia, didn’t catch it from us and she’s still antibody negative. I don’t know how that happened, since she lives with us and we all live in a tiny Columbia apartment together. But 2 or 3 people in my environment at work ended up catching it, one way or another, from me or from someone else, I don’t know. But it lingered for about 6 weeks. Looking back, it was very textbook. It’s just that when I caught it, not much was known about the symptoms; we didn’t know the difference between this or flu. And I did get antibody tested as part of the healthcare providers. I got an early antibody test and it was positive, so a positive antibody test together with all these obvious symptoms pretty surely means I had it. Anyway, I asked all of my students if any of them had it. Of course, none of them had been tested, but none of them had any symptoms more than a 3 day sniffle or something. Last question here: what is your perspective on the future—I know you talked a bit about this regarding your research, but also the broader impacts of COVID-19 on science in general, and society as well? When this first started, I was traveling to China a lot up until that point. I had been working there a lot. On my Facebook page (another use of the cloud by the way, since I use it to store my massive quantities of travel photos), I had a blog going. Mid-January, just from what I gleaned from the press and the talk, I said there’s this new virus that has every making of a pandemic. I don’t know how I knew that in mid-January and our president didn’t know that until mid-March, but whatever [laughs]. We had plenty of warning. I said there’s this new virus coming out of Wuhan; people don’t know whether it’s coming from a dead fish or a live mammal (a bat) or a snake. At the time they were saying it was a type of snake called a krait or cobra. So they don’t know whether it’s coming from a reptile or a dead fish or a live bat. If scientists can’t recognize this thing, I know our body isn’t going to recognize it, and if our bodies can’t recognize it, this is pandemic material. Sure enough, here we are. At the beginning of February, I noted in my blog the World Health Organization working together with scientists in China and scientists around the world, including the US. I was very impressed with the way the world, together with the World Health Organization, was working together across borders to get a handle on this virus very quickly. I saw real cooperation and I commented on that in a very hopeful way, because on so many issues, the world doesn’t work together and can’t cooperate. Countries like South Korea have become a model of cooperation and positive action. I know people fault China for getting a slow start and trying to control the PR on this thing just like our own country did, but they did respond strongly and correctly and were able to stop this thing in its tracks in a very largely populated part of the world. So I did see real models of cooperation, following science and medicine and accordingly, and getting positive results from that. We do have recorded examples of what working together across borders in science and medicine can accomplish for all of us. Unfortunately, as you see, especially in our own country, this cooperation rapidly devolved and (I’m happy to be on public record for this) because of our lousy leadership, we see an example of the human tragedy that bad leadership, a lack of coordinated government response, and a lack of international collaboration in goodwill can cause. So this disease has produced examples of both—the best and the worst of world cooperation in science and medicine to confront a world problem. I think we’ll be able to look back at COVID collectively and learn very important lessons across the broad spectrum of what to do and what not to do. I hope we will learn.
By: Hannah Lin (CC '23)
Can you describe your COVID-19 research at the moment? I am a cardiologist focused on heart arrhythmias, which is electrophysiology. I’m a clinician, so I see patients, I do surgeries, I do procedures, but I’m also a physician-scientist, so my main career is research on animal models of heart arrhythmias that affect humans. My specializations include atrial fibrillation, as well as ventricular arrhythmias such as ventricular tachycardia and ventricular fibrillation. My career is not focused on COVID research. I am funded by the National Institute of Health for my studies on the mechanisms of heart arrhythmias in humans, which I am working on in mice. I have a special imaging laboratory that images the electrical activations of the heart, so it is not COVID-specific. You may have read on the news that what were thought to be possible treatment modalities for COVID, such as hydroxychloroquine, can lead to heart arrhythmias. That is where my clinical work became involved in COVID research--looking at heart arrhythmias in patients who are and are not treated with hydroxychloroquine. Some patients, even without treatment with hydroxychloroquine or azithromycin, have heart arrhythmias. I published a paper during this COVID pandemic that is now in circulation--Arrhythmia and Electrophysiology, on the cardiac arrhythmias that affect patients with COVID. Some of the heart arrhythmias that patients with COVID-19 experience include atrial fibrillation, and that’s due to the lack of oxygen because of lung failure--ARDS, or acute respiratory distress syndrome. They also experience other things such as atrioventricular block, so the node that connects the atrium to the top of the heart in the ventricle, is malfunctioned. Patients with COVID-19 unfortunately, towards the end of their disease due to multi-organ dysfunction, have what we call pulseless electrical activity, so the heart may have some electrical activity, but there’s actually no heart contraction to deliver a pulse. Unfortunately, that leads to death. One of the heart arrhythmias that patients on hydroxychloroquine and azithromycin can experience due to the prolonged QT interval, which is the repolarization of the heart when we see it on the electrocardiogram, is something called QT prolongation. And that’s something that’s been reported. We are analyzing data on measuring the QT interval in patients with and without COVID-19 being treated with hydroxychloroquine, and also doing research on the heart arrhythmias that patients with COVID-19 have. Are you still enrolling patients in studies? We are conducting a retrospective chart review on patients who have COVID-19 and comparing them to patients who were COVID-tested but were negative, so who don’t have COVID-19. And we want to see what the difference is between the heart arrhythmias in patients with and without COVID-19. What is special about COVID-19 and heart arrhythmias? It is a retrospective trial, so we’re looking back. Now, as you know, the number of patients is decreasing, thankfully, so it is not a prospective trial. So this is ongoing? It is ongoing research, but not ongoing enrollment. What is the general timeline of your research right now? When do you think this retrospective review will be over? All COVID research is time sensitive because it’s highly competitive and people want information as soon as possible. We are working as fast and as hard as we can. Has there been anything in your research in the past few months that has surprised you? I think that the underlying mechanisms in which COVID-19 causes severe sickness in patients is really unclear. I think all of the specialists--virologists, cardiologists, nephrologists, endocrinologists, pulmonologists--we’re all learning about this disease. I don’t think anyone can claim that we know exactly how it works. If we did, we would have more treatment modalities for it. One thing we’re definitely learning is that COVID-19 can affect many organs, the heart being one of them. Obviously, it is a team approach between different specialists to take care of a patient with COVID-19, because they can develop not only lung problems but also heart problems as well as kidney problems and blood problems like blood clots. It’s really a multi-systemic disorder. Is your team still keeping prior research projects going while you engage in this COVID research? Yes. I think that’s the difficulty of being a physician as well as a scientist. So there’s clinical work that obviously is COVID-19, but as a scientist, I’m trying to understand cardiac arrhythmias, even before COVID-19 happened, why and when cardiac arrhythmias occur. That is still ongoing. Are you still seeing patients through telemedicine? Yes, I think all of us have been and I have been even during the surge. I worked at the hospital during the surge and I was doing televisits to take care of patients who were at home and not at the hospital. I think one of the great things about electrophysiology or being a heart arrhythmia doctor is a lot of our devices, like pacemakers and defibrillators and monitors, they all do remote downloads. The patient does not need to be physically in my clinic or in the hospital for me to check on how they’re doing. They have a remote monitoring device where the device downloads information from their monitor wirelessly and it gets sent to our clinic for review within the same day--the longest is 24 hours. That is one great thing about advanced technology--it allows us to remotely monitor these patients. They do not need to be physically in front of us. Can you talk about your experience of working in the hospital during the surge? One, I’m very thankful for the Columbia New York Presbyterian Hospital leadership. It was truly exceptional, and they had constant transparent communication about the number of patients in the hospital and how they were preparing staff and the hospital facility to take care of these patients. I think that there was also exceptional teamwork, especially in the beginning of the surge, when there were obviously a lot of sick patients coming in. Although our colleagues in Asia and Europe had a lot of experience with COVID-19, we were still learning on our own if there were any differences in the patients in America compared to all the patients internationally, if it all presented the same way. I think we were all very shocked as to how the infection could attack so many parts of the body. It really called to all of our abilities to take care of these sick patients. I am very proud of a lot of the trainees--the medical students and residents and fellows who were on the frontlines, how we all worked together. All those things were key in addition to keeping calm under such intense pressure, teamwork, and constant communication to support one another and how to improve care to COVID-19 patients while protecting ourselves. Are there any common misconceptions you’ve heard regarding COVID-19 that you would like to rectify or respond to? A couple of things: physicians who have taken care of these patients know that it can really happen to anybody. It is not only older patients or patients with preexisting conditions. They are the majority of patients, but we’ve seen very sick patients who were young and without any prior health conditions. And it is not just the flu. There was a flu vaccine, whereas there isn’t a COVID-19 vaccine as of yet. It is contagious, and also COVID-19 has a lot of sequelae; it attacks many organ systems. Patients that we saw were much sicker than those with the common flu. What is your perspective on the future--both in terms of your research and the broader impacts of COVID-19? I think this is a great time for students and trainees to pursue a career in research. COVID-19 has shown that scientists and research are essential. The only way to really overcome this disease is healthcare workers taking care of these patients and advancement in science to develop treatment modalities. I think it’s very inspiring for me as a physician-scientist and I feel very privileged that I can be both a physician to take care of patients and also engage in science research to try to understand the mechanisms of COVID infection and hopefully develop new treatments for patients with arrhythmias due to COVID infection. It’s a really good time to re-engage students in the importance of doing scientific research and considering a career in science. Being a physician-scientist is difficult because you are doing three jobs everyday: being a teacher, doing research, and taking care of patients. But it is very important that we have specialists who understand what you see in the clinic or the hospital taking care of patients and also being able to translate this to perform science to understand what’s going on underneath it all. |